Abstract
Foodborne diseases (FBDs) are a major public health concern, especially in Sub-Saharan African (SSA) countries, such as Ghana, where poor food handling practices (FHPs) are prevalent. To estimate the pooled proportion of good FHPs and the associated factors among Ghanaian food handlers, this systematic review and meta-analysis was conducted to aid scholars, practitioners and policymakers in devising FBD-preventable interventions. The scientific databases PubMed, Google Scholar, Science Direct, African Journals Online, ProQuest, and Directory of Open Access Journals were systematically searched until April 19, 2023, for relevant literature. Observational studies meeting the inclusion criteria of reported good FHPs among food handlers were included. Three authors independently searched the database, assessed the risks of bias and extracted the data from the shortlisted articles. A random-effects model with the DerSimonian and Laird model was used to estimate the pooled effect size of FHPs and the pooled odds ratio (POR) of FHP-associated factors. Out of the 2019 records collated, 33 with a total sample size of 6095 food handlers met the inclusion criteria for meta-analysis. The pooled proportion of good FHPs among Ghanaian food handlers was 55.8% [95% Cl (48.7, 62.8%); I2 = 97.4%; p < 0.001]. Lack of food safety training [POR = 0.10; 95% CI (0.03, 0.35); p = 0.001] and inadequate knowledge of food hygiene [POR = 0.36; 95% CI (0.01, 10.19); p < 0.001] were identified as the critical good FHP-associated factors. The study showed that the proportion of good FHPs among Ghanaian food handlers was 55.8%. To increase knowledge of food hygiene among food handlers, the Ghanaian Food and Drugs Authority (FDA) is recommended to provide regular training on food safety for the well-being of the general public.
Introduction
In light of the various endemic infectious diseases, the health infrastructure and the associated food-handling practices in Ghana need critical consideration1,2. These include food processing and manufacturing facilities, storage and logistics services, as the majority of infectious diseases either emerge or spread through the consumption of unhygienic food with unacceptable levels of food safety hazards3,4. In the face of the prevailing low economic conditions and poor health infrastructure, it is prudent to practise all preventive measures through good food handling practices (FHPs) that could ensure safe food and drastically reduce the risk of foodborne diseases (FBDs)5,6.
FHPs are a collective key measure primarily to maintain biological food safety during storage, processing, preparation and the hygiene of cooking utensils as well as other surfaces that are likely to come in direct contact with food7,8. Poor FHPs across all economies are responsible for 75% of FBD outbreaks, resulting in approximately 420,000 deaths each year6,9. Research reveals that 18% of all FBD deaths were associated with food being contaminated by food handlers6. Food handlers are individuals who are directly in contact with food storage, preparation and packaging, as well as with food-handling utensils8,10.
Studies have shown that training in food safety6,8,10, food hygiene attitudes8,10, educational level6,8,10, knowledge of food hygiene8, average monthly income6 and registration of food handlers and their medical fitness6,8,10 are associated with good FHPs. Systematic reviews and meta-analyses conducted in Ethiopia revealed that the pooled good FHPs among food handlers ranged between 48.410 and 50.5%8. The proportion of good FHPs among Ghanaian food handlers based on individual observational studies ranged between 24.419 and 87.0%2. Frequent FBD outbreaks such as diarrhoea, cholera and typhoid in Ghana are presumably directly associated with poor FHPs and poor environmental sanitation11,12,13.
Researchers and policymakers need empirical evidence in decision-making. However, observational studies of individual research groups on the estimated proportion of FHPs in Ghana are inconsistent for an informed decision. Given these gaps, it was necessary to undertake a systematic review and meta-analysis of FHPs in Ghana to adequately evaluate them. This review considers good FHPs to be the reported standard FHPs classified as ‘good’ based on statistical analyses. Good FHP ensures that the food for consumption is largely safe from biological hazards2,4,6.
A meta-analysis was therefore conducted to pool the proportion of good FHPs among Ghanaian food handlers to generate a single summary estimate from several independent studies by pooling the data. It increases the sample size, detects publication biases and leads to more precise estimates of the proportion while identifying deficiencies in study design, data analyses and interpretation of the findings. Estimating the pooled proportion of good FHPs and the associated factors among Ghanaian food handlers was the primary objective to aid scholars, practitioners and policymakers in devising FBD-preventable interventions.
The findings could also help health authorities and agencies such as the Food and Drugs Authority (FDA), especially in Ghana, to implement good FHPs among food handlers to prevent FBDs. Furthermore, this review could be beneficial for international agencies such as the World Health Organization (WHO) and the Food and Agriculture Organization (FAO) of the United Nations (UN) to develop an effective global food safety plan.
Methods
This systematic review and meta-analysis report followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines14. The protocol that was followed is registered on PROSPERO (ID: CRD42022352777).
Search strategy
Relevant literature was searched online on PubMed, Google Scholar, Science Direct, African Journals Online, ProQuest, and the Directory of Open Access Journals for the available published articles until April 19, 2023, using ‘food’, ‘foods’, ‘handling practice’, ‘hygiene practice’, ‘hand hygiene’, ‘safety practice’, ‘food hygiene’, ‘food handling’, ‘food safety’, ‘food sanitation’, ‘professional practices’, ‘associated factors’, ‘identified factors’, ‘factors associated’, ‘determinant factors’, ‘factors contributing’, ‘food handlers’, ‘food vendors’, ‘street food vendors’ and ‘Ghana’ as keywords and Medical Subject Headings (MeSH). A complete list of the search keywords and the strategies adopted are detailed in the supplementary file (Tables 1, 2). In addition to the database search, the cited literature listed in the reference of the articles was also manually searched, and the relevant additional articles were identified and included.
Eligibility criteria
Random studies on food handlers operating in food catering establishments, institutions and roadside/streets were included. Observational studies on cross-sectional, case–control and cohort studies that reported the proportion of good FHPs (or provided data on good FHPs of food handlers for which the proportion could be calculated as the primary outcome) were included. The shortlisted articles included those published across the timeline in the English language and excluded inaccessible full-text articles where several attempts to communicate with the corresponding authors failed. It also excludes articles where it was difficult to extract the needed data of the primary objective, i.e., the proportion of good FHPs. Additionally, studies outside Ghana and articles with ambiguous methodologies were also excluded.
Quality assessment of the shortlisted studies
Three authors independently assessed the quality of the studies and resolved the discrepancies that arose through consensus. The Joanna Briggs Institute (JBI) quality assessment tool for prevalence studies was adopted to assess the quality of the shortlisted studies/data and the risks of bias15. The JBI tool was chosen because it helped assess the methodological quality of a study and determine the extent to which a study has addressed the possibility of bias in its design, conduct and analysis15. It also aided in reducing information overload by eliminating irrelevant and/or weak studies and allowed the identification of the most relevant work15. The tool comprises nine parameters focusing on the appropriate sampling frame, proper sampling technique, adequate sample size, study subject and setting description, sufficient data analysis, use of valid methods to identify conditions, validation of all participants, use of appropriate statistical analysis and adequate response rate. The risks of bias were classified based on the total score; a score of 0 was assigned if the parameters coincided and 1 if they did not. The risk was low with a score of ≤ 2, moderate at 3–4, or high at ≥ 5. Only the articles with low and moderate risks of bias were included, as detailed in Table 3 in the supplementary file. Disagreements, if any, were resolved through discussion and consensus.
Screening, selection, and data extraction from the shortlisted studies
Mendeley desktop Ver. 1.19.6 was used to import all the references from the searched database. Three authors used Rayyan software to screen the title, abstract, full text and study selection. A standard extraction format was used to extract the necessary data, such as first author, publication year, region, study design, sampling method, sample size, response rate and good FHP proportions (the standard FHPs reported in the individual studies classified as good based on the categorization of the statistical analyses were considered good FHPs). For instance, hygiene practices of 37.1% were classified as ‘poor’ and 62.9% as ‘good’ by Tuglo et al.6. ‘Good hygiene practices’ were extracted from all the included literature. Any screening, study selection, and data extraction disagreements were resolved through consensus.
Statistical analyses
Data were analysed using STATA software version 17. The heterogeneity of the dataset was assessed using Cochran’s Q test and I2 statistic with the corresponding p values. The random-effects model with the DerSimonian and Laird (DL) model was used to estimate the pooled effect size of FHPs and the pooled odds ratio (POR) of the FHP-associated factors. A leave-one-out sensitivity analysis was conducted to assess the strength and influence of each study on the overall effect size estimate. A funnel plot was used visually to assess publication bias in conjunction with statistical methods such as the regression-based Egger test and Begg’s rank correlation tests (p < 0.05) for confirmation. Subgroup analysis and meta-regression were conducted to identify potential sources of heterogeneity in the pooled proportion estimates.
Results
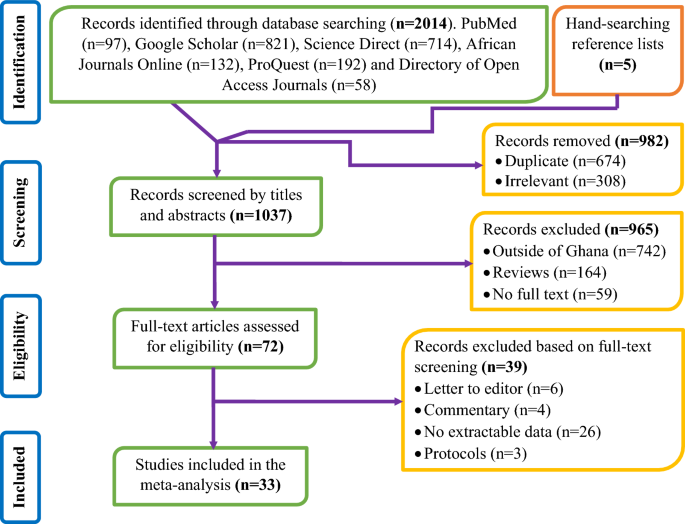
Database searches of the relevant studies yielded 2014 records, and manual searching from the lists of references yielded an additional five records. A total of 1037 titles and abstracts were screened after removing 982 duplicate and/or irrelevant records and excluding an additional 965 records without full texts, and 72 full-text records were considered for data assessment. Of these, 39 articles were finally excluded where incoherence was discovered during data assessment, and the data of 33 studies were meta-analysed (Fig. 1).

PRISMA flow diagram specifying the considerations to exclude and include the articles.
Characteristics of the shortlisted studies
The 33 studies2,4,6,7,11,12,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42 included were published between 2009 and 2022 and were cross-sectionally designed with a total of 6095 food handlers. Six major studies were carried out in the Greater Accra2,20,27,28,35,38 and Volta6,11,23,25,30,32 regions, and five were carried out in the Northern region12,21,34,40,41. Eighteen studies2,6,7,12,16,19,21,22,23,25,28,30,32,33,34,36,41,42 used a simple random sampling technique, and4,20,26,27,38,39 used systematic sampling (18.2%; n = 6) (Table 1).
Risk of bias in the included studies
Regarding the quality of the included studies, eight studies4,6,11,20,22,26,34,40 had a low risk of bias (24.2%), and 25 studies2,7,12,16,17,18,19,21,23,24,25,27,28,29,30,31,32,33,35,36,37,38,39,41,42 had a moderate risk of bias (75.8%) (Supplementary File Table 3, on pages 2 and 3).
Meta-analysis
The pooled proportion of good FHPs from the meta-analysis on Ghanaian food handlers was 55.8% (95% CI 48.7, 62.8%). The heterogeneity across studies was high and significant [(I2 = 97.4%); p < 0.001)]. Based on the included studies, the highest proportion of good FHPs was 87.0% (95% CI 83.0, 91.0%), as reported by Dun-Dery et al.2, and the lowest was 24.4% (95% CI 17.3, 31.5%), as reported by Amaami et al.19 (Fig. 2).

Forest plot of the proportion of good FHPs among food handlers in Ghana.
Sensitivity analysis
To estimate the influence of individual studies on the overall meta-analysis, a sensitivity analysis was performed. The pooled data meta-analysis results were close to the actual effect size, which ranged from 54.7% (95% CI 47.8, 61.7%; p < 0.001) to 56.8% (95% CI 49.8, 63.8%; p < 0.001), even after the removal of a single study at a time, suggesting that no single included study had an overwhelming effect on the pooled estimate of good FHPs (Fig. 3).

Sensitivity analysis of the proportion of good FHPs among food handlers in Ghana.
Subgroup analysis
The proportion of good FHPs in studies reported in or after 2020 was 59.5% (95% CI 48.3, 70.8%), and the same was 53.5% (95% CI 43.8, 63.3%) in studies reported earlier. The proportion of good FHPs was 57.1% (95% Cl 48.6, 65.7%) in studies using probability sampling, while it was 51.8% (95% CI 41.0, 62.5%) in studies that did not. The proportion of good FHPs was 60.1% (95% CI 40.8, 79.3%) among studies having > 300 and 54.9% (95% CI 47.2, 62.7%) among studies having ≤ 300 sample sizes. Studies assessed as having low risks of bias showed a high (59.2%) proportion of good FHPs (95% CI 48.4, 70.1%) compared with moderate (54.6%) risks of bias (95% CI 45.4, 63.8%). All the subgroups had substantial heterogeneity. The heterogeneity of good FHP estimates for each subgroup could not be explained, as the results in individual articles were inconsistent (Table 2).
Meta-regression
Meta-regression was executed using variables such as the year of publication, sample size, response rate and risk of bias score to identify potential sources of heterogeneity. Bivariate and multivariable analyses showed insignificant sources of heterogeneity among them (p > 0.05; Table 3).
Publication bias
The visible symmetric funnel shape plot suggested that there was no publication bias (Fig. 4). The regression-based Egger test (p = 0.378) and Begg’s rank correlation test (p = 0.486) meta-analyses confirmed that there was no publication bias among the included studies.

Funnel plot of studies with risk bias of the proportion of good FHPs among Ghanaian food handlers.
Factors associated with FHPs among Ghanaian food handlers
Four out of 33 included studies6,30,39,40 reported FHP-associated factors (Table 4). Three studies6,30,40 reported an association between a lack of food safety training and good FHPs. The pooled estimate indicated that the odds of abiding by good FHPs were 0.10× lower among the nontrained food handlers than among their trained counterparts (POR = 0.10; 95% CI 0.03, 0.35; p = 0.001; Fig. 5). Two studies39,40 reported that inadequate knowledge of food hygiene and good FHPs were associated. The POR showed that food handlers with inadequate knowledge of food hygiene were 0.36× less likely to adhere to good FHPs than those with adequate knowledge (POR = 0.36; 95% CI 0.01, 10.19%; p < 0.001; Fig. 6).

Forest plot of the association between lack of food safety training and good FHPs in Ghana.

Forest plot of the association between inadequate knowledge of food hygiene and good FHPs in Ghana.
Discussion
The majority of FBDs are often associated with poor FHPs6. This meta-analysis showed 55.8% good FHPs among the Ghanaian food handlers, implying that the recommended personnel hygiene, utensils and surroundings cleaning and appropriate food storage being crucial in food poisoning and FBDs reduction were complied with. This finding could be attributed to adequate food hygiene training, proper infrastructure and adequate supervision by regulatory agencies such as the FDA. Educational campaigns and action-oriented interventions before and after food safety training by the FDA and monitoring the effects could improve FHPs and ensure food safety at the consumer level.
Consistent with our findings, an earlier meta-analysis (50.5%) by Zenbaba et al.8 was reported among Ethiopian food handlers. The pooled estimate in the present study was higher than the 48.4% figure of Negassa et al.10, who carried out a pooled good FHP meta-analysis in Ethiopia. The disparities across the studies are attributable to environmental and cultural differences, access to food safety training, varying knowledge of food hygiene and the frequency of supervision by the enforcement agencies. A systematic review reported 72.7% poor FHPs among Bangladeshi food handlers43, wherein the discrepancy could be due to the diverse study setting and sociodemographic characteristics among the food handlers. Food establishments operate without formal food safety training, registration to operate food business or regular medical check-ups and fitness tests of the food handlers in most developing countries6,30,40.
The heterogeneity among the included literature was significant, as reflected through analyses of the subgroup ‘year of publication’ and the sampling method. The significant statistical heterogeneity arising from the methodological differences in subgroup analyses suggested that all the studies did not estimate the same quantity but does not necessarily suggest that the effect of the pooled estimate size varied. A high proportion of good FHPs was seen in studies published after 2020. This anomaly is attributable to the individual good FHP proportions included in the meta-analysis, sampling method and differences in the study setting. Another reason could be that FBD prevention measures during the COVID-19 pandemic, as enforced by the WHO, warranted adherence to personnel hygiene44 in line with the WHO’s five keys to safe food5. The meta-analysis in the subgroup ‘probability sampling’ had a high proportion of good FHPs compared to its nonprobability counterpart. This disparity is attributed to the varying sociodemographic characteristics of food handlers and the sampling techniques adopted.
A training of food handlers usually seeks to impart two major transformations, to acquire adequate knowledge and skillsets and to help translate the knowledge into practice6. The pooled odds ratio showed that food handlers with no food safety training were less likely to follow good FHPs than those who underwent them. This finding is corroborated by two earlier FHP meta-analyses conducted among Ethiopian food handlers8,10, which concluded that trained food handlers were more likely to follow good hygiene practices than untrained food handlers8,10. The training helped them gain accurate knowledge of good FHPs. Therefore, food handlers must receive frequent and effective training in food safety to ensure good FHPs under the cGMP (current Good Manufacturing Practices) requirements (Fig. 7).

The quality assurance pyramid that defines and ensures the highest order of food safety.
As per the present meta-analysis, food handlers with inadequate knowledge of food hygiene were less likely to adhere to good FHPs than those with adequate knowledge. This concurs with an earlier Ethiopian meta-analysis that found that food handlers with good food hygiene knowledge were more likely to apply good FHPs than their ignorant counterparts8. Poor FHPs could critically affect the health of food consumers, with severe food poisoning and consequently the spread of FBDs; hence, our finding affirms the recommendation by the WHO11 of frequent assessment of FHP knowledge to prevent FBDs.
Strengths and limitations
This is the first systematic review and meta-analysis on food safety and hygiene practices in the Ghanaian context to provide a pooled estimate of good FHPs and the associated factors to aid in the implementation of feasible FHP compliance and interventions among food handlers. Like any other scientific investigation, it has its limitations. First, the study was cross-sectional in design without permitting discrepancies between the cause and the effect. Second, the good FHP proportions extracted from the shortlisted literature were based on the reporting as presented, which might have a social desirability bias. Third, there were variations among the studies without a standard definition for ‘good FHPs’. Fourth, only articles published in the English language were included, excluding vernacular language literature.
Summary of the finding
Any good food processing or manufacturing facility in modern times should ideally have cGMP and Hazard Analysis Critical Control Point (HACCP) in place in compliance with the food safety standards, the former occupying the base and the latter occupying the peak of the food safety (quality assurance) pyramid. The former focuses primarily on the training to be provided to the food handlers, and the latter focuses on analysing the possible physical, chemical or biological hazards that are likely in the food being processed (Fig. 7).
Conclusions
The study showed that the proportion of good FHPs among Ghanaian food handlers was 55.8%. Lack of food safety training and inadequate knowledge of food hygiene were identified as good FHP-associated factors. To increase knowledge of food hygiene among food handlers, the FDA in Ghana is recommended to provide regular training on food safety for the well-being of the general public. The FDA should also be strict on food safety regulations among food handlers through surveillance and frequent monitoring systems to prevent frequent outbreaks of FBDs such as diarrhoea, cholera and typhoid in Ghana. Further studies in Ghana should focus on strong study designs such as cohort and interventional studies in reporting FHPs and should associate the adverse findings, if any, with region-specific FBD outbreaks.
Data availability
The manuscript contains all pertinent information.
Abbreviations
- FBDs:
-
Foodborne diseases
- SSA:
-
Sub-Saharan African
- FHPs:
-
Food handling practices
- POR:
-
Pooled odds ratio
- DL:
-
DerSimonian‒Laird
- CI:
-
Confidence interval
- FDA:
-
Food and Drugs Authority
- WHO:
-
World Health Organization
- COVID-19:
-
Coronavirus disease 2019
- cGMP:
-
Current good manufacturing practice
- SSOP:
-
Sanitation standard operating procedure
- SOP:
-
Standard operating procedure
- HACCP:
-
Hazard analysis critical control point
- QMS:
-
Quality management system
- ISO:
-
International Organization for Standardization
References
-
Mohapatra, R. K. et al. Recent surge in cholera outbreaks globally during the COVID-19 pandemic era: A potential threat to the African continent and salient counteracting strategies. Int. J. Surg. 109, 631–633 (2023).
Google Scholar
-
Oduro-Yeboah, C., Ackah, N. B., Akonor, P. T., Amponsah, S. K. & Mboom, F. P. Food safety knowledge and practices among fresh coconut vendors. Sci. Afr. 8, 1–6 (2020).
-
Mohapatra, R. K., Kutikuppala, L. V. S., Mishra, S., Tuglo, L. S. & Dhama, K. Rising global incidence of invasive group A Streptococcus infection and scarlet fever in the COVID-19 era–our knowledge thus far. Int. J. Surg. 109, 639–640 (2023).
Google Scholar
-
Odonkor, S. T. & Odonkor, C. J. A. An assessment of food safety knowledge and practices in the Ghanaian hospitality industry. J. Food. Qual. 1, 1–9 (2020).
Google Scholar
-
Tuglo, L. S. et al. Sociodemographic characteristics and reproductive health factors associated with maternal knowledge and practice of infection prevention in neonates in North Dayi District, Ghana. Front. Public Health 11, 1–10 (2023).
Google Scholar
-
Tuglo, L. S. et al. Food safety knowledge, attitude, and hygiene practices of street-cooked food handlers in North Dayi District, Ghana. Environ. Health Prev. Med. 26, 1–13 (2021).
Google Scholar
-
Addo-Tham, R., Appiah-Brempong, E., Vampere, H., Acquah-Gyan, E. & Gyimah, A. A. Knowledge on food safety and food-handling practices of street food vendors in Ejisu-Juaben Municipality of Ghana. Adv. Public Health 1, 1–7 (2020).
Google Scholar
-
Zenbaba, D. et al. Food hygiene practices and determinants among food handlers in Ethiopia: A systematic review and meta-analysis. Trop. Med. Health. 50, 1–15 (2022).
Google Scholar
-
Mohapatra, R. K., Mishra, S. & Tuglo, L. S. Surge in iatrogenic botulism cases in Europe: Threat perceptions and salient countering measures. New Microbes New Infect. 53, 1–2 (2023).
Google Scholar
-
Negassa, B., Ashuro, Z. & Soboksa, N. E. Hygienic food handling practices and associated factors among food handlers in Ethiopia: A systematic review and meta-analysis. Environ. Health Insights 16, 1–9 (2022).
Google Scholar
-
Madilo, F. K., Letsyo, E. & Klutse, C. M. A cross-sectional study on food safety knowledge and practices among food handlers in tertiary and second circle institutions in Ho municipality, Ghana. Food Sci. Nutr. 11, 778–793 (2023).
Google Scholar
-
Ziblim, S.-D. & Yakubu, A. Knowledge of food hygiene practices among street food vendors in Sagnarigu municipality of Ghana: A cross sectional study. J. Food Microbiol. Saf. Hyg. 7, 1–7 (2022).
-
Tuglo, L. S. et al. The association between pregnancy-related factors and health status before and after childbirth with satisfaction with skilled delivery in multiple dimensions among postpartum mothers in the Akatsi South District, Ghana. Front. Public Heal. 9, 1–12 (2022).
-
Page, M. J. et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 10, 1–11 (2021).
Google Scholar
-
Higgins, J. P. T. et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomized trials. Bmj 343, 1–9 (2011).
Google Scholar
-
Bigson, K., Essuman, E. K. & Lotse, C. W. Food hygiene practices at the Ghana school feeding programme in wa and cape coast cities. J. Environ. Public Health. 1, 1–7 (2020).
Google Scholar
-
Mwini, G. A. & Tuolienuo, C. Street food venders’ perspectives of hygiene practices of street food vendors in basic schools in Sissala East District of Ghana. J. Educ. Pract. 9, 1–9 (2018).
-
Boakye, N. A. B., Boateng, N. A. D. & Hagan, J. A. Assessing the hygienic state of hospital kitchens in the Sekondi-Takoradi Metropolis of Ghana. Eur. J. Hosp. Tour. Res. 3, 1–9 (2016).
-
Antwi, E. A. Assessment of personal and food hygiene practices of food handlers in educational institutions in the Kwawu-East District of Ghana: Assessment of personal and food hygiene practices of food handlers in educational institutions in the Kwawu-East District, Ghana. J. Health Phys. Educ. Recreat. Sport Danc. 10, 1–15 (2017).
-
Donkor, E. S., Kayang, B. B., Quaye, J. & Akyeh, M. L. Application of the WHO keys of safer food to improve food handling practices of food vendors in a poor resource community in Ghana. Int. J. Environ. Res. Public Health 6, 2833–2842 (2009).
Google Scholar
-
Adzitey, F., Sulleyman, K. W. & Kum, P. K. Knowledge and practices of meat safety by meat sellers in the Tamale Metropolis of Ghana. Food Prot. Trends 40, 40–47 (2020).
-
Gyebi, B. E. A., Annan, R. A., Apprey, C., Asamoah-Boakye, O. & Asare, C. Y. Knowledge, attitude, and practices (KAP) of foodservice providers, and microbial quality on food served in Kumasi. J. Foodserv. Bus. Res. 24, 397–413 (2021).
Google Scholar
-
Dah, H. M. Exploring the hygienic practices among kitchen staff in the training college of education: The case of Hohoe. Food Sci. Qual. Manag. 51, 59–69 (2016).
-
Nartey, E., Owusu, J., Gamor, E. & Mensah, E. E. Assessment of knowledge and practices of food hygiene and safety of caterers in senior high schools in Ghana: A case study of two senior high schools in Koforidua. ADRRI J. Agric. Food Sci. 3, 1–18 (2017).
-
Appietu, M. E. & Amuquandoh, E. F. Examining food safety knowledge and the microbiological quality of school meals in Ghana. Afr. J. Hosp. Tour. Manag. 2, 1–15 (2020).
-
Akabanda, F., Hlortsi, E. H. & Owusu-Kwarteng, J. Food safety knowledge, attitudes and practices of institutional food-handlers in Ghana. BMC Public Health 17, 1–9 (2017).
Google Scholar
-
Kunadu, A.P.-H., Ofosu, D. B., Aboagye, E. & Tano-Debrah, K. Food safety knowledge, attitudes and self-reported practices of food handlers in institutional foodservice in Accra, Ghana. Food Control 69, 1–27 (2016).
-
Ovai, B., Akunzule, A. N. & Kunadu, A.P.-H. Assessment of the subjective food safety knowledge, attitudes and practices of informal live bird traders in Accra, Ghana. Food Prot. Trends 39, 62–73 (2019).
-
Dwumfour-Asare, B. Effect of local authorities’ field monitoring visits on awareness of regulation and hygiene practices among street food vendors: The case of two district capitals in Ghana. J. Behav. Health 4, 71–80 (2015).
Google Scholar
-
Frempong, C. S., Charles-Unadike, V. O., Anaman-Torgbor, J. A. & Tarkang, E. E. Correlates of intention to practice good food hygiene among street food-vendors in Kadjebi District, Ghana. Int. J. Health Promot. Educ. 1, 1–13 (2022).
Google Scholar
-
Amaami, A. J., Dominic, D. & Collins, D. Factors associated with poor food safety compliance among street food vendors in the Techiman Municipality of Ghana. Afr. J. Food Sci. 11, 50–57 (2017).
Google Scholar
-
Bormann, F., Adzinyo, O. & Letsa, L. Safety and hygiene status of street vended foods in Ho, Ghana. J. Hosp. Manag. Tour. 7, 25–32 (2016).
Google Scholar
-
Monney, I., Agyei, D., Ewoenam, B. S., Priscilla, C. & Nyaw, S. Food hygiene and safety practices among street food vendors: An assessment of compliance, institutional and legislative framework in Ghana. Food public Health 4, 306–315 (2014).
-
Apanga, S., Addah, J. & Sey, D. R. Food safety knowledge and practice of street food vendors in rural Northern Ghana. Food Public Health 4, 99–103 (2014).
-
Odonkor, S. T., Adom, T., Boatin, R., Bansa, D. & Odonkor, C. J. Evaluation of hygiene practices among street food vendors in Accra metropolis, Ghana. Elixir Food Sci. 41, 5807–5811 (2011).
-
Dajaan, D. S. et al. Food hygiene awareness and environmental practices among food vendors in basic schools at Kintampo township, Ghana. Food Public Health 8, 13–20 (2018).
-
Annan-Prah, A., Mensah, A. A., Akorli, S. Y., Asare, P. T. & Kumi-Die, I. D. Slaughterhouses, animal slaughter and slaughter hygiene in Ghana. J. Vet. Adv. 2, 189–198 (2012).
-
McArthur-Floyd, M., Commey, V. & Boakye, N. A. B. Evaluation of food safety among fast food operators in Madina, Accra. Food Sci. Qual. Manag. 54, 18–25 (2016).
-
Dun-Dery, E. J. & Addo, H. O. Food hygiene awareness, processing and practice among street food vendors in Ghana. Food Public Health 6, 65–74 (2016).
-
Amegah, K. E. et al. Determinants of hand hygiene practice at critical times among food handlers in educational institutions of the Sagnarigu Municipality of Ghana: A cross-sectional study. Environ. Health Insights 14, 1–10 (2020).
Google Scholar
-
Danikuu, F. M., Baguo, F. B. & Azipala, O. Hygiene practices among street food vendors in Tamale Metropolis. J. Med. Biomed. Sci. 4, 25–30 (2015).
Google Scholar
-
Monney, I., Agyei, D. & Owusu, W. Hygienic practices among food vendors in educational institutions in Ghana: The case of Konongo. Foods 2, 282–294 (2013).
Google Scholar
-
Rifat, M. A., Talukdar, I. H., Lamichhane, N., Atarodi, V. & Alam, S. S. Food safety knowledge and practices among food handlers in bangladesh: A systematic review. Food Control 142, 1–10 (2022).
Google Scholar
-
Agyekum, B. A. & Tuglo, L. S. Effect of COVID-19 on dental care for children during the postpandemic era in Ghana: A concern for policymaking. Front. Dent. Med. 4, 1–6 (2023).
Google Scholar
Author information
Authors and Affiliations
Contributions
L.S.T., S.M., R.K.M., N.K.K., J.N.A., H.M., Q.L. and S.N.D. contributed to the conception and protocol design. M.P.K., A.T.P., J.D.T., T.C., S.M.S., K.S.A. and A.D. evaluated the methodological quality of the studies included. L.S.T., S.M., R.K.M., N.K.K., J.N.A., H.M., Q.L., S.N.D. and A.D. participated in the data extraction, analysis and interpretation. All authors involved in the writing of the first draft, editing, corrections and final approval of the submitted manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary Information.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Reprints and Permissions
About this article
Cite this article
Tuglo, L.S., Mishra, S., Mohapatra, R.K. et al. A systematic review and meta-analysis of food handling practices in Ghana vis-a-vis the associated factors among food handlers during 2009 and 2022.
Sci Rep 13, 18748 (2023). https://doi.org/10.1038/s41598-023-46150-8
-
Received: 13 July 2023
-
Accepted: 27 October 2023
-
Published: 31 October 2023
-
DOI: https://doi.org/10.1038/s41598-023-46150-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.