Abstract
This study aimed to examine the association of hemoglobin concentration with a 90-day mortality of young adult patients with ICH in a large retrospective cohort. A retrospective observational study was conducted between December 2013 and June 2019 in two tertiary academic medical centers in China. We defined patients with hemoglobin concentration 160 g/L as high hemoglobin. Associations of hemoglobin and outcomes were evaluated in multivariable regression analyses. The primary outcome was mortality at 90 days. We identified 4098 patients with ICH who met the inclusion criteria. After adjusting primary confounding variables, the 90-day mortality rate was significantly higher in young patients with severe anemia (OR, 39.65; 95% CI 15.42–101.97), moderate anemia (OR, 2.49; 95% CI 1.24–5.00), mild anemia (OR, 1.89; 95% CI 1.20–2.98), and high hemoglobin (OR, 2.03; 95% CI 1.26–3.26) group than in young patients of the normal group. The younger age was associated with a higher risk of death from anemia in patients with ICH (P for interaction = 0.01). In young adult patients with ICH, hemoglobin concentration was associated with 90-day mortality, and even mild to moderate anemia correlated with higher mortality. We also found that in ICH patients with anemia, younger age was associated with higher risk.
Introduction
Intracerebral hemorrhage (ICH) is a common cause of stroke (15–30%), which affects about 2.5 per 10,000 people each year, and only 20% of survivors are functionally independent at 6 months1,2. ICH patients with comorbidities, such as severe anemia, are likely to have a poor prognosis and be admitted to an intensive care unit3,4.
Although evidence has demonstrated that anemia is associated with poor outcomes in patients with ICH5, however, age differences in the association need to be more fully characterized. ICH and anemia are more common in the elderly, but there is still a large amount of young adult ICH patients with anemia (from 12.9 to 31%)6,7,8. The capacity of younger adults to increase cardiac output is considerably higher than that of older adults9, and regulation of cerebral oxygenation alters with increasing age10. This evidence suggests that youth have more tolerance for a reduction in Hb. Moreover, several guidelines recommend that transfusion be not only based on the hemoglobin concentration but also on consideration of overall clinical status, of which age is one of the important factors11. Advancements in our understanding of the relationship between age, anemia, and outcomes in patients with ICH may potentially inform the successful development of blood transfusion services.
The objectives of this study were to examine the association of hemoglobin concentration with a 90-day mortality of young adult patients with ICH in a large retrospective cohort. We hypothesized both low and high hemoglobin concentrations on admission were associated with high mortality in young adult patients with ICH.
Methods
Study design and setting
This is a retrospective, observational study based on consecutively electronic health records from West China Hospital Sichuan University between December 2010 and July 2019 and the First of People’s Hospital of Longquanyi District between January 2017 and October 2020. This study was approved by both West China Hospital and the First of People’s Hospital of Longquanyi District Institutional Review Board. All authors had no access to information that could identify individual participants during or after data collection.
Participants
Patients through the following were included for further analysis: (1) radiologically confirmed case of acute primary (non-traumatic) ICH, (2) no history of previous ICH, (3) follow-up data available at 90 days.
Patients were excluded if they met the critical exclusion criteria: (1) traumatic ICH, (2) acute ischemic stroke, (3) subarachnoid hemorrhage, (4) subdural hemorrhage, (5) first computed tomography (CT) digital imaging and communication not available in electronic medical records, (6) unavailable hemoglobin concentration at admission.
Patients younger than 50 were defined as young adult patients, and older than 50 were defined as elderly patients.
Hemoglobin on admission
We used hemoglobin on admission as the exposure factor in this study. As per the guideline of WHO12, the diagnosis of anemia in men was based on a hemoglobin of less than 130 g/L; in women, it was less than 120 g/L. Multiple guidelines recommend the hemoglobin threshold for red blood cell transfusion is 70–80 g/L for adults. Thus, we defined patients with hemoglobin concentration 160 g/L as high hemoglobin.
Outcomes
The primary outcome was mortality at 90 days. Secondary outcomes were mortality at 30 days, 1 year, and the longest follow-up.
We retrieved the whole death records up to August 15, 2021, for further analysis via the Household Registration Administration System from the Department of Public Security, Sichuan Province, China. China’s law demands that once a citizen dies, the head of household, relatives, dependents, or neighbors shall report the death registration to the household registration authority and cancel the household registration within 1 month. This system has accurate death records. Therefore, it was negligible for the rate of loss to follow up this study.
Statistical analysis
Continuous variables were presented as mean ± standard deviation (SD), and categorical variables were reported with frequencies and percentages to describe the baseline characteristics of enrolled patients. The missing values have been replaced by mean values.
Univariable logistic regression analysis was performed to assess the association of baseline characteristics with favorable outcomes. Confounders included in the multivariable regression models were derived from previous relative studies and clinical expertise, including age, gender, smoking, alcohol abuse, hypertension, diabetes, size of the hematoma, infratentorial hematoma, intraventricular hematoma, Glasgow Coma Scale (GCS). We used restricted cubic spline functions to analyze the log-linearity assumption for continuous characteristics. Then, factors associated with a value of P < 0.10 in univariate analyses were implemented into the multivariable logistic regression model. We also performed subgroup comparisons between patients with low hemoglobin concentration and normal hemoglobin concentration at admission by age stratification.
Kaplan–Meier analyses and log-rank tests were used to examine all-cause mortality after ICH amongst different subgroups of hemoglobin concentration. Cox’s proportional hazards model was used to adjust for major potential confounders and estimate hazard ratios (HR) for survival.
P values less than 0.05 were set as the threshold for statistical significance, and all P values were 2-sided. R statistical software (version 4.1.3; Foundation for Statistical Computing) was used to perform all statistical analyses.
Ethical statement
This is a retrospective study based on medical records and has been granted an exemption from requiring written informed consent by the ethics committee of West China Hospital (No. 20211701) and the ethics committee of the First of People’s Hospital of Longquanyi District (No. 2022004). This study complied with the guidelines for human studies and was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Results
Of the 7013 patients diagnosed with ICH in the above two medical hospitals. After excluding criteria, a total of 1290 young adult patients (the age from 18 to 50 years) and 2808 elderly patients (> 50 years) were included in this study. A flowchart of patient selection is shown in eFigure 1. The demographic characteristics of recruited patients are shown in Table 1 (the detailed characteristics of young adult and elderly patients were shown in eTable 1 and eTable 2). Among the 1290 young adult patients, 360 (28%) had anemia on admission (Hb concentration: < 120 for females, < 130 for males). Patients with lower hemoglobin concentration were more likely to be female and presented with fewer smokers and alcohol abusers, more hypertension, larger hematoma, and a decline in GCS (P < 0.05).
Univariate and multivariable analysis results are summarized in Table 2 to demonstrate the associations between hemoglobin of admission and mortality at 90 days. After adjusting for confounders (age, smoking, hypertension, size of hematoma, intraventricular hematoma, GCS, operation of hematoma), the 90-day mortality rate was significantly higher in young adult patients with severe anemia, mild to moderate anemia, and high hemoglobin group than the normal group (Severe anemia versus normal: adjusted odds ratio (aOR), 39.65; 95% CI 15.42–101.97; moderate anemia versus normal: aOR, 2.49; 95% CI 1.24–5.00, mild anemia versus normal: aOR, 1.89; 95% CI 1.20–2.98, high hemoglobin versus normal: aOR, 2.03; 95% CI 1.26–3.26). We found the association between hemoglobin concentration and 90-day mortality were more obvious in young adult patients than elderly (The aOR in young patients: 39.65 (15.42–101.97) versus the aOR in elder patients: 3.35 (1.79–6.30)). As shown in Fig. 2, with the graded decrease in hemoglobin concentrations, the risk of death gradually increased.
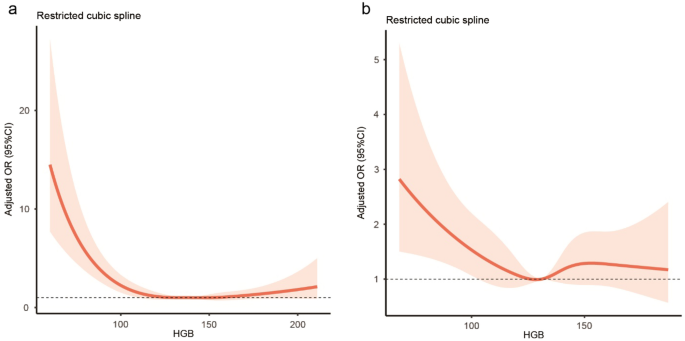
The restricted cubic spline was used to visualize the association of hemoglobin concentration with 90-day mortality. A nonlinear association between Hb and 90 days mortality was presented in Fig. 1 (P for non-linearity < 0.001)13,14. We set a Hb cutoff of 140 g/L in the young adult patient group and found both below and above the cutoff showed a strong and graded association between Hb concentration and mortality (below the cutoff: adjusted OR 0.47, 95% CI 0.38–0.59, for each 1-SD Hb increase; above the cutoff: adjusted OR 1.72, 95% CI 1.36–2.17, for each 1-SD Hb increase). When hemoglobin was analyzed as continuous, the adjusted OR of 90-day mortality for each 1-SD increase in hemoglobin was 0.71 (95% CI 0.61–0.84).

Relationship between hemoglobin and 90-day mortality in patients with ICH. (a) Young adult patients, (b) elderly patients.
We conducted subgroup analysis by age stratification on hemoglobin concentration with a cutoff value of 130 g/L, and we found that the mortality was higher in young ICH patients with anemia (Fig. 2, P for interaction = 0.01). The Kaplan–Meier curves indicated that either lower or higher hemoglobin concentration of admission was associated with higher mortality after ICH (P < 0.0001; Fig. 3). Furthermore, we collected serial hemoglobin measurements of patients in ICH after admission. Similar results of mortality at 30 days, 1 year, and the longest follow-up were shown in eTable 3 in the appendix. During hospital admission within the first week, the hemoglobin concentration of those who died was generally lower than those who survived (eFigure 2; P < 0.001).

Subgroup analysis of the association between hemoglobin concentration and 90-day mortality in age stratification.

Kaplan–Meier survival curves indicating the relationship between admission hemoglobin and 90-day mortality after ICH. (a) Young adult patients, (b) elderly patients.
Discussion
In this cohort study, we found both low and high hemoglobin concentrations on admission indicated poor outcomes in young adult patients with ICH. The survival analysis showed even mild to moderate anemia correlated with higher mortality. Subgroup analysis showed that the effect of anemia on mortality increases with decreasing age.
Extensive researchers have reported the association of anemia with the mortality of ICH patients. Miguel et al. demonstrated the association of anemia on admission with greater intracerebral hemorrhage severity, higher mortality, and worse functional outcomes11. Meanwhile, Tiffany et al. suggested that nadir hemoglobin could also be used to predict poor functional outcomes of ICH patients15,16,17. All the above studies have specifically emphasized the importance of anemia in the outcome of patients with ICH.
The reason for anemia-related mortality in ICH patients is complex, and age is one of the most important factors16,18. Previous studies indicated the etiologies and risk factors of anemia at younger ages are different from those in older people. Compared with elderly patients, young adult patients were more likely with clonal disorders of hematopoiesis, yet the vast majority of elderly patients with nutritional deficiency anemias resulting from chronic systemic syndromes such as renal insufficiency19,20. The damage of anemia in young adult patients was more severe than in other age stratification. Therefore, the results of cohort studies in elderly patients cannot directly be translated to apply to younger individuals.
However, none of these studies focused on young adult ICH patient groups. Multiple large retrospective studies indicated the etiology, diagnosis, and prognosis of anemia in young adults and the elderly are different21. Besides these differences, choosing young adult patients as the study sample could reduce the confounding effects of age, such as mild anemia caused by the age-associated decline in renal function or in testosterone concentrations22. To our knowledge, this research was the first large cohort study to conduct the association of anemia with the prognosis in young adult ICH patients. We found both low and high hemoglobin concentration on admission associated with poor outcomes in young adult ICH patients, and even mild to moderate anemia correlated with higher mortality. Within the first week after admission, the trajectory of hemoglobin concentration showed a continuous downward trend, which indicates the necessity of early intervention of anemia among young adult patients with ICH. As shown in Fig. 3, risk of death seems to stabilize in younger patients early whereas it continues to decline in older patients as time passes. That may be due to deaths from other causes in older individuals such as advanced cancers.
Our study represents the largest study of young adults to date. A total of 1290 young adults and 2808 elderly ICH patients with anemia were included in cohorts. Each sample contains detailed medical records and accurate death records, which are extracted from household registration data. There are some aspects of the implications in this study. First, including younger patients allows for a more comprehensive understanding of the disease’s impact across different age groups. By comparing outcomes between younger and older patients, researchers can more accurately gauge the disease’s progression and its potential influence on mortality rates. Second, although the causes of anemia and causes of death cannot be provided, it is still valuable to collect data on younger patients. This data could help clinicians better understand the prognosis and potential outcomes for younger patients with ICH. By building a more comprehensive dataset across age groups, healthcare providers can make more informed decisions regarding treatment options, patient monitoring, and prognosis discussions. While it is true that causes of anemia and causes of death cannot be provided, the inclusion of younger patients can still contribute to a more thorough understanding of mortality following ICH.
There are also some limitations in this study. First, although we adjusted for confounding factors by multivariable logistic regression, there might be several unobserved confounders, such as etiology, time of admission, and surgical intervention. Second, the outcome of this study did not contain functional outcomes such as the modified Rankin Scale. Thirdly, we did not distinguish between acute and chronic anemia in patients with ICH. Fourth, due to the inherent limitations of retrospective clinic studies, the causes of anemia, causes of death, rates of blood transfusion, and other severe comorbidities (advanced cancer) are not identifiable in the data presented.
Conclusions
In this large study, we collected 1290 young adults and 2808 elderly patients with ICH and found that hemoglobin concentration on admission was associated with 90-day mortality. Those results indicated both low and high hemoglobin concentrations on admission presented negative effects and even mild to moderate anemia correlated with higher mortality in young adult patients with ICH. Compared to older age, we found that the mortality was higher in young ICH patients with anemia. Further studies may be conducted on early intervention of anemia in young adult patients with ICH.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
-
Diedler, J. et al. Low hemoglobin is associated with poor functional outcome after non-traumatic, supratentorial intracerebral hemorrhage. Crit. Care 14(2), R63 (2010).
Google Scholar
-
Vermeer, S. E. et al. Long-term prognosis after recovery from primary intracerebral hemorrhage. Neurology 59(2), 205–209 (2002).
Google Scholar
-
Zhang, S. et al. Associations of anemia with outcomes in patients with spontaneous intracerebral hemorrhage: A meta-analysis. Front. Neurol. 10, 406 (2019).
Google Scholar
-
Yen, C. C. et al. Recurrent primary intracerebral hemorrhage: A hospital based study. Acta Neurol. Taiwan 16(2), 74–80 (2007).
Google Scholar
-
Kellert, L. et al. Anemia in young patients with ischaemic stroke. Eur. J. Neurol. 22(6), 948–953 (2015).
Google Scholar
-
Namaganda, P. et al. Stroke in young adults, stroke types and risk factors: A case control study. BMC Neurol. 22(1), 335 (2022).
Google Scholar
-
Mustapha, A. F., Sanya, E. O. & Bello, T. O. Stroke among young adults at the LAUTECH Teaching Hospital, Osogbo, Nigeria. Niger. Q. J. Hosp. Med. 22(3), 177–180 (2012).
Google Scholar
-
Hoffmann, M. Stroke in the young: The multiethnic prospective durban stroke data bank results. J. Stroke Cerebrovasc. Dis. 7(6), 404–413 (1998).
Google Scholar
-
Simon, G. I. et al. Impacts of aging on anemia tolerance, transfusion thresholds, and patient blood management. Transfus. Med. Rev. 33(3), 154–161 (2019).
Google Scholar
-
Beishon, L. et al. Vascular and haemodynamic issues of brain ageing. Pflugers Arch. 473(5), 735–751 (2021).
Google Scholar
-
Melgaard, L. et al. Age dependence of risk factors for stroke and death in young patients with atrial fibrillation: A nationwide study. Stroke 45(5), 1331–1337 (2014).
Google Scholar
-
WHO/UNICEF/UNU. Iron Deficiency Anaemia: Assessment, Prevention, and Control (World Health Organization, 2001).
-
Zakai, N. A. et al. A prospective study of anemia status, hemoglobin concentration, and mortality in an elderly cohort: The Cardiovascular Health Study. Arch. Intern. Med. 165(19), 2214–2220 (2005).
Google Scholar
-
Graham, F. J. et al. Assessment of haemoglobin and serum markers of iron deficiency in people with cardiovascular disease. Heart 109(17), 1294–1301 (2023).
Google Scholar
-
Chang, T. R. et al. Nadir hemoglobin is associated with poor outcome from intracerebral hemorrhage. Springerplus 2, 379 (2013).
Google Scholar
-
van Asch, C. J. et al. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: A systematic review and meta-analysis. Lancet Neurol. 9(2), 167–176 (2010).
Google Scholar
-
Togha, M. & Bakhtavar, K. Factors associated with in-hospital mortality following intracerebral hemorrhage: A three-year study in Tehran, Iran. BMC Neurol. 4, 9 (2004).
Google Scholar
-
Schepers, V. P. et al. Functional recovery differs between ischaemic and haemorrhagic stroke patients. J. Rehabil. Med. 40(6), 487–489 (2008).
Google Scholar
-
Poon, M. T., Fonville, A. F. & Al-Shahi Salman, R. Long-term prognosis after intracerebral haemorrhage: Systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry 85(6), 660–667 (2014).
Google Scholar
-
Koivunen, R. J. et al. Incidence, risk factors, etiology, severity and short-term outcome of non-traumatic intracerebral hemorrhage in young adults. Eur. J. Neurol. 22(1), 123–132 (2015).
Google Scholar
-
Hemphill, J. C. 3rd. et al. The ICH score: A simple, reliable grading scale for intracerebral hemorrhage. Stroke 32(4), 891–897 (2001).
Google Scholar
-
Gupta, M. et al. Perihematomal edema as predictor of outcome in spontaneous intracerebral hemorrhage. J. Neurosci. Rural Pract. 5(1), 48–54 (2014).
Google Scholar
Funding
This work is supported by National Natural Science Foundation of China (82271364) (Yu Zhang), the innovation team project of Affiliated Hospital of Clinical Medicine College of Chengdu University (CDFYCX202203) (Yu Zhang), and the project of Sichuan Science and Technology Bureau (22ZDYF0798) (Fang Fang), the 1·3·5 project for disciplines of excellence-Clinical Research Incubation Project, West China Hospital, Sichuan University (21HXFH046) (Fang Fang), and Nursing Association of Sichuan Province H21003 (Chao Huang).
Author information
Authors and Affiliations
Contributions
Study concept: F.F. Design: All authors. Acquisition, analysis, or interpretation of data: Y.X. and Y.Z. Statistical analysis: Y.X. and Y.Z. Drafting of the manuscript: Y.X. and Y.Z. Critical revision of the manuscript for important intellectual content: All authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Supplementary Information.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Reprints and Permissions
About this article
Cite this article
Tian, Y., Zhang, Y., He, J. et al. Association of anemia with mortality in young adult patients with intracerebral hemorrhage.
Sci Rep 13, 19711 (2023). https://doi.org/10.1038/s41598-023-46941-z
-
Received: 29 December 2022
-
Accepted: 07 November 2023
-
Published: 12 November 2023
-
DOI: https://doi.org/10.1038/s41598-023-46941-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.