Abstract
This study evaluated the efficacy of a blended teaching model integrating real-life scenarios into nutrition education for nursing students. The study adhered to the CONSORT guidelines. Participants (N = 283) were cluster-randomized into two groups: a blended teaching group (n = 76) receiving self-management activities via WeChat Moments alongside teachers, and a traditional teaching group (n = 207) receiving teacher-based instruction. A battery of survey items was meticulously analyzed, including demographics, educational quality, self-directed learning ability, and the willingness to further study in the nutrition course. Additionally, chapter test scores, final examination grades, nutritional counseling capabilities, and final course grades were evaluate. Blended teaching significantly improved the chapter test average (P = 0.018), willingness to continue learning (P = 0.018), students’ evaluation of teaching quality (P = 0.027), and nutritional counseling capabilities (P < 0.001); however, no differences were observed in final exam grades (P = 0.620) or final course grades (P = 0.951). Our research findings clearly show that combining blended teaching with real-life scenarios significantly benefits educational quality. It boosts students’ willingness to keep learning, their evaluation of teaching quality, and their self-directed learning awareness, and also favorably impacts the development of their nutritional counseling capabilities.
Introduction
Teaching approaches are changing and evolving in higher and medical education. The literature increasingly reports that the use of digital educational technologies has rapidly expanded, becoming a priority for many academic higher education institutions, especially during the COVID-19 pandemic1,2,3. Digital education plays an essential role in medical education4,5,6. Blended teaching is a reinforcement of teaching through digital Internet technology in traditional courses7. It can be an effective teaching strategy and seems to have excellent long-term development potential compared to traditional face-to-face teaching8. The current study defines blended learning as a combination of traditional face-to-face teaching and online practicing/learning7,9. Traditional teaching follows a teacher-centered model that allows students to passively accept new knowledge, lacking active learning10. Blended learning is a student-centered teaching model8; it blends the advantages of traditional teaching and the convenience and abundant resources of the Internet11. Studies have revealed that traditional education can no longer adapt to the current requirements of education12,13. However, a literature review shows that the effectiveness of blended learning remains controversial. The outcome variables compared were exam grades, learning satisfaction, and learners’ ability to apply newly acquired knowledge or skills11. Most studies have shown that blended teaching is more effective than traditional teaching14,15,16,17,18, while the results of some studies are not statistically significant19,20. Hence, it is necessary to continue researching blended teaching.
Nurses assume a pivotal role in the provision of nutritional counseling within the realm of patient health education21,22,23. However, recent evidence underscores critical gaps in nursing students’ foundational and applied nutritional knowledge. For instance, a scoping review systematically examined nutrition education interventions for nursing students and identified a pressing need to integrate digital platforms and active learning strategies to enhance clinical relevance and skill retention23. This aligns with prior findings that nursing curricula often prioritize theoretical content over practical skill development, leaving students ill-equipped to address real-world dietary challenges24. Similarly, studies reported that nursing students frequently struggle to translate classroom-acquired nutritional concepts into actionable counseling strategies, particularly in culturally diverse settings25,26. Recent advancements in clinical nutrition education emphasize the integration of digital tools and active learning to bridge this gap. For example, Almendingen et al. demonstrated that a flipped classroom model combined with digital case-based learning significantly improved nursing students’ ability to address malnutrition in clinical scenarios27. Similarly, Mancin et al. reported that active teaching methodologies, such as audience response systems and case discussions, enhanced nutritional knowledge retention among first-year nursing students28. Further supporting this, Thang et al. highlighted the efficacy of blended learning approaches (e.g., teaching kitchens and service-based learning) in fostering practical nutrition skills among interdisciplinary healthcare trainees29. These findings resonate with broader trends in nursing education. Our research focuses on nutrition courses in nursing education, aiming to explore the impact of a blended teaching model on learning outcomes and nutritional counseling capabilities. By incorporating self-management activities via a digital platform (WeChat Moments) into traditional teaching, we aim to provide a foundation for improving teaching methodologies in nursing education. This approach aligns with emerging trends in clinical nutrition education, where blended models integrating digital tools and active learning strategies have shown promise in enhancing students’ practical competencies. In this study, self-management is defined as students’ independent application of nutritional knowledge through the digital platform, involving dietary analysis and evaluation, thereby facilitating self-regulation of their nutritional learning to achieve superior learning outcomes and real-life application.
This study erects a theoretical scaffolding predicated on the constructivist learning theory and the social learning theory. The constructivist learning theory accentuates the process through which learners actively fabricate knowledge30. In the context of blended teaching, students actively amalgamate the acquired nutritional knowledge with real-life scenarios by means of online self-management undertakings and offline traditional instruction, thereby forging their own comprehension and application proficiencies of nutritional knowledge. Illustratively, when students disseminate pictures of their dietary intakes on WeChat Moments and proffer comments premised on classroom-learned knowledge, this procedure galvanizes them to engage in profound cogitation regarding food nutrition combinations, consequently augmenting their understanding of the subject matter. The social learning theory elucidates the modus operandi by which students assimilate healthy eating behaviors and nutritional knowledge through the observation and emulation of others (feedback and exemplifications from peers and teachers) during the sharing and deliberation process31. In blended teaching, students engage in reciprocal observation and learning within group activities and online interactions. For example, in classroom group presentations, students can garner novel perspectives and methodologies from their peers’ reports, and during WeChat Moments sharing and discussions, they can glean insights from others’ healthy eating experiences, thereby perpetually refining their own nutritional knowledge frameworks and laying the groundwork for the augmentation of nutritional counseling capabilities. The principal outcomes of this study encompassed students’ evaluations regarding educational quality and nutritional counseling capabilities. Meanwhile, the secondary outcomes comprised examination grades, self-directed learning ability, and the willingness to further study in the nutrition course.
Methods
Participants
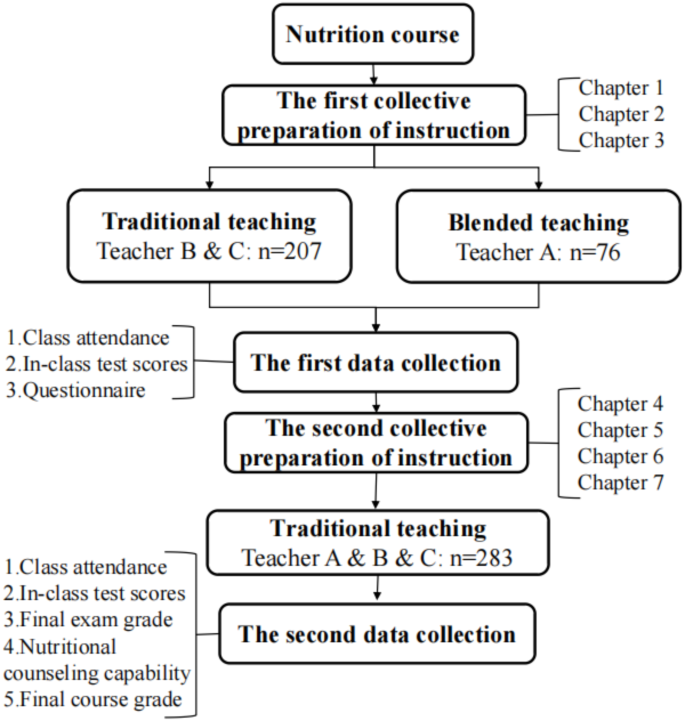
This cluster-randomized trial adhered to the CONSORT guidelines. This study was conducted within a nutrition course tailored for undergraduate nursing students. Three teachers (Teacher A, B, C) were randomly designated to oversee the nursing students. The participation in this study was entirely voluntary, and no particular benefits were provided to the students. A total of 283 undergraduate nursing students from 11 classes were enrolled in this study. To minimize selection bias, participants were allocated to two teaching groups through cluster randomization, with the administrative class serving as the randomization unit. The 11 classes were grouped into three administrative clusters as follows: Cluster 1 (Classes 1–4), Cluster 2 (Classes 5–8), and Cluster 3 (Classes 9–11). Subsequently, clusters were randomly assigned to either the blended teaching group or the traditional teaching group. The blended teaching group comprised three classes (76 students) supervised by Teacher A, while the traditional teaching group included eight classes (207 students), evenly distributed between Teachers B and C (four classes per teacher). The teachers engaged in collaborative lesson planning for both the initial three and the final four chapters of the course curriculum, with the principal objective of pinpointing the crucial and challenging aspects. For the first three chapters of the nutrition course, the traditional teaching approach and the blended teaching methodology were respectively implemented among different groups of students. In contrast, solely the traditional teaching method was uniformly employed for the last four chapters. The final four chapters focused on clinical nutrition topics (e.g., disease-specific nutritional interventions). However, as our study emphasized self-practice in foundational nutrition (e.g., weight management), disease-specific content was excluded from blended teaching activities. Future studies will explore innovative formats for implementing nutritional interventions in disease-specific contexts to enhance practical applicability.
Structure and settings of different teaching approaches
In the context of traditional teaching, specific requirements were established for pre-class, in-class, and post-class activities. The in-class requirements were obligatory, whereas those for pre-class and post-class were discretionary. Pre-class, students were mandated to peruse the teacher’s courseware and the relevant textbook chapters. During in-class sessions, following the completion of each chapter’s course content, a test was administered. The test incorporated a variety of question types and was to be completed independently. Throughout the entire course, a cumulative total of seven tests were distributed. These tests were disseminated via teaching process assistant tools, and the results were obtainable instantaneously upon submission. Subsequently, the teacher elucidated the common issues that emerged from the tests. The crucial in-class elements were centered around the significant and challenging points identified through collaborative lesson planning. Post-class activities mainly extended to the reading of peer-reviewed and popular science articles. Blended teaching incorporated traditional teaching and self-management activities. The self-management activities were predominantly carried out after class. Students were randomly allocated to distinct groups. WeChat Moments groups were formed, which were only accessible to group members and teacher A. Within these groups, students shared images of their meals and provided comments regarding the suitability of the food in light of what they had learned in class. During each class, one group of students would deliver a 5-minute presentation on the content and inadequacies of a particular student’s three meals within the group. All groups presented in sequential order.
Data collection and instruments
A survey was implemented among the students, with data collection occurring at two specific time points: subsequent to the third week of the course and on the final day of the course. For the initial data collection, the following elements were involved: class attendance, in-class test scores (for the first three chapters), and a questionnaire which encompassed basic information, the student evaluation of educational quality scale, and a self-directed learning ability scale. Regarding the second data collection, it consisted of class attendance, in-class test scores (for the last four chapters), final examination grades, nutritional counseling capabilities as manifested by the scores of a comprehensive essay question in the final examination, and final course grades. The teaching process assistants were responsible for gathering student class attendance, in-class test scores (with one test administered per chapter), and final exam scores. The initial data collection incorporated a voluntary questionnaire. A total of 283 questionnaires were distributed through the Internet, and all were completed in their entirety. The flowchart of this study, as well as the calculation of the final course score, were presented in meticulous detail in Figs. 1 and 2.

The flowchart.
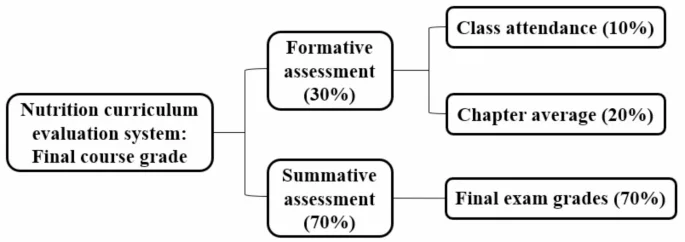
Nutrition curriculum evaluation system.
The student evaluation of educational quality (SEEQ) scale represents a reliable and valid instrument furnished with independent subscales, which is specifically designed for the context of higher education32. It has been extensively validated and authenticated on an international scale within the domain of medical education33,34. This scale encompasses 32 items, which are further categorized into nine distinct dimensions, namely learning, enthusiasm, organization, group interaction, individual rapport, breadth, examinations, assignments, and overall. Students were instructed to assign a rating to each item on a five-point scale, with the options being strongly disagree [1], disagree [2], neutral [3], agree [4], and strongly agree [5]. The scale spans from 32 to 160 points, where a higher score is indicative of superior educational quality.
The self-directed learning ability (SDL) scale was evaluated by means of a rating scale formulated by Williamson35. This scale consisted of 60 items, which were partitioned into five dimensions, namely awareness, learning strategies, learning activities, evaluation, and interpersonal skills. Students were required to provide a rating for each item on a five-point scale, with the descriptors being always [1], often [2], sometimes [3], seldom [4], and never [5]. The scale extended from 60 to 300 points, wherein a lower score corresponded to a more proficient SDL capability.
Data analysis
Statistical analyses were carried out with the utilization of SPSS version 23.0. Categorical variables were presented in the form of numbers and percentages, whereas numerical variables were depicted as means and standard deviations. The differences among numerical variables were examined by means of t-tests. Pearson’s coefficients were employed to delineate the correlations between the variables. The level of statistical significance was established at P ≤ 0.05.
Study protocol approval.
This study was conducted in accordance with the Helsinki Declaration and its recent modifications. All students who participated in this study were adults and had been clearly informed of the study’s nature and purpose. They voluntarily participated and provided informed consent in writing before any data collection began. The study underwent ethical review and obtained approval from the School of Public Health at Wannan Medical College (approval number: LL-2021jyxm43).
Results
Demographic data
This study incorporated 283 nursing students for the purpose of data analysis. Given that the nursing profession was the focus of this study, the proportion of female students was 75.6%. Over half (61.8%) of the participants resided in rural areas. Subsequent to obtaining new knowledge from the nutrition course, all participants exhibited a notably high level of willingness to continue learning, with a mean score of 8.71 ± 1.64. The demographic details of the participants are illustrated in Table 1.
Scores for different periods
As previously stated, in the first three chapters of the nutrition course, both traditional and blended teaching methods were employed, while in the last four chapters, only traditional teaching was utilized. As presented in Table 2, all students demonstrated a strong willingness to continue learning; nevertheless, a significant disparity was detected (P = 0.018). The test results for Chaps. 1 to 3 indicated a remarkable difference between blended teaching and traditional teaching (P < 0.001, P = 0.046, and P = 0.036, respectively). A significant divergence was also identified in the Chap. 4 test (P = 0.050) and the average chapter test (P = 0.018). However, no distinctions were observed in Chaps. 5–7, the final examination grade, and the final course grade. Additionally, all students attained full marks for class attendance.
Self-directed learning ability (SDL)
We assessed the SDL ability of all students during the third week. As presented in Table 3, no significant difference was found in the total scores between the blended and traditional teaching methods (P = 0.298). Among the five dimensions of SDL, a significant difference was solely detected in the dimension of awareness (P = 0.021), whereas no differences were identified in learning strategy, learning behavior, evaluation, and interpersonal skills (P = 0.641, P = 0.429, P = 0.451, and P = 0.751, respectively).
Student evaluation of educational quality (SEEQ)
Educational quality was assessed during the third week. The total score of SEEQ for blended teaching was markedly higher than that of traditional teaching (P = 0.027), indicating that blended teaching corresponded to superior educational quality. These advantages were primarily manifested in the learning (P < 0.001), enthusiasm (P = 0.007), organization (P = 0.023), and overall evaluation (P = 0.011) aspects of the course and the teacher. No significant differences were detected in the other SEEQ dimensions (as shown in Table 4).
Correlation analysis
We examined the associations between the overall and total scores of SEEQ and the scores of different periods as well as the willingness to continue learning. As presented in Table 5, a robust correlation was identified between the overall and total SEEQ scores (r = 0.849, P < 0.01). Both exhibited a positive correlation with the average chapter test score and the willingness to continue learning, yet no significant association was detected with the final examination grade or the final course grade. Intriguingly, students’ willingness to continue learning did not display a significant correlation with their grades in different periods. In essence, students who favored blended teaching were more inclined to continue learning, although this was not manifested in their final grades.
Our previous data showed differences in SDL awareness across teaching groups; therefore, we further explored the correlation between SDL awareness and SEEQ dimensions. As shown in Table 6, a strong positive correlation was observed between all dimensions of the SEEQ. SDL awareness showed a significant positive relationship with several dimensions of the SEEQ, such as learning, enthusiasm, organization, examinations, assignments, overall, and total scores (r = -0.149, r = -0.129, r = -0.153, r = -0.123, r = -0.149, r = -0.143, and r = -0.143, respectively; the lower the score, the better the SDL capability).
Our prior data had revealed differences in SDL awareness among teaching groups; thus, we further probed the correlation between SDL awareness and the SEEQ dimensions. As depicted in Table 6, a strong positive correlation was observed among all SEEQ dimensions. SDL awareness demonstrated a significant positive relationship with several SEEQ dimensions, including learning, enthusiasm, organization, examinations, assignments, overall, and total scores (r = -0.149, r = -0.129, r = -0.153, r = -0.123, r = -0.149, r = -0.143, and r = -0.143, respectively).
Discussion
This study aimed to evaluate the efficacy of a blended teaching model integrating real-life scenarios into nutrition education for nursing students, focusing on enhancing learning outcomes, self-directed learning awareness, and nutritional counseling capabilities. Our findings demonstrate that blended teaching significantly improved students’ engagement, practical knowledge application, and willingness to continue learning, aligning with emerging trends in digital and active learning methodologies within nursing education.
Self-management necessitates the transformation of book-derived knowledge into practical implementation by means of constructing real-life scenarios, and this is of fundamental significance for the development of nutritional counseling capabilities. Individuals with concerns regarding their health and self-management could enhance their personal initiatives by leveraging the learned knowledge36. Our results resonate with recent studies emphasizing the integration of digital tools in nursing education. For instance, Almendingen et al. demonstrated that digital case-based learning significantly improved nursing students’ ability to translate theoretical knowledge into clinical practice, mirroring our findings on enhanced nutritional counseling capabilities27. Similarly, Mancin et al. highlighted that active teaching methodologies foster deeper engagement and knowledge retention, corroborating our observed improvements in educational quality and student enthusiasm28.
The effectiveness of blended teaching in fostering self-directed learning aligns with advancements in digital education frameworks. A 2025 systematic review by Dogan et al. underscored the critical role of blended learning in addressing gaps in nursing students’ nutritional competencies23. This role is particularly evident through platforms enabling real-time interaction and peer feedback-a feature central to our WeChat Moments activities. Furthermore, Thang et al. reported that active pedagogy enhanced interdisciplinary trainees’ practical skills, supporting our emphasis on real-life scenario integration29.
In this study, it was noted that the blended teaching group achieved significantly higher total SEEQ scores and outperformed the traditional group in four dimensions: learning, enthusiasm, organization, and overall evaluation (Table 4). The total score functions as an indicator of students’ comprehensive appraisal of the teaching quality of the course37. These outcomes are consistent with the broader adoption of active learning strategies in nursing education. For example, Huang et al. found that blended models incorporating Google Classroom improved clinical pathology course evaluations, paralleling our results on organizational and enthusiasm dimensions17. Evidently, this implies that the students within the blended teaching group possess a greater level of recognition regarding the teaching quality of the nutrition course, which can be explained from the following four dimensions. The learning dimension primarily focuses on assessing students’ perception of the learning content and its significance within the course context. Specifically, it aims to determine whether students deem the course conducive to their knowledge acquisition and ability augmentation. In the blended teaching approach, students are furnished with enhanced flexibility and autonomy in structuring their learning process. They can participate in online activities according to their own paces. Such a self-regulated learning mode facilitates students’ understanding and internalization of the learning content. Moreover, the practical application scenarios incorporated in the blended teaching framework augment the value of learning, as students can directly perceive the relevance and practicality of the acquired knowledge. The enthusiasm dimension chiefly measures the teacher’s enthusiasm level during the teaching process and assesses whether it can effectively kindle students’ interest in learning. In the context of the enthusiasm dimension, the diverse teaching methods employed in blended teaching can substantially enhance teacher enthusiasm and, in turn, stimulate student interest. For example, online platforms like WeChat Moments provide an avenue for students to actively participate and exchange ideas. This active learning milieu not only showcases the teacher’s enthusiasm but also serves to arouse students’ interest, rendering them more engaged in the learning process compared to traditional lecture-oriented teaching. The organization dimension pertains to the rationality of the organizational arrangements in course teaching, encompassing aspects such as the structure of the teaching content and the teaching progress management. For instance, online activities enable teachers to identify areas requiring more attention and then restructure the teaching content. Offline activities can be designed to supplement and reinforce the online learning, ensuring a more logical and efficient course progression. This, in turn, leads to a more favorable perception of the course organization among students. The overall dimension, a crucial comprehensive evaluation aspect of the entire teaching quality, takes into account multiple factors and elicits students’ overall perception and evaluation of the course. In the overall dimension, the blended teaching approach combines online and offline resources to provide a more comprehensive and integrated learning experience, enabling students to have a more holistic understanding of the course. Consequently, students within the blended teaching group are more likely to attain higher scores in these four dimensions, thereby contributing to the elevation of the total score of the SEEQ scale.
A systematic review concluded that digital problem-based learning was potentially more effective in improving knowledge and skills owing to increased student interaction and engagement38. A recent study conducted in Thailand has demonstrated that the implementation of a blended problem-based learning approach integrated into online flipped classrooms significantly enhances students’ problem-solving skills and academic achievement39. Our research also identified significant differences in SDL awareness, willingness to continue learning, and nutritional counseling capabilities among different teaching groups. Blended teaching highlights application, particularly the nutritional counseling abilities. The blended teaching mode creates a real-life application scenario by allowing students to share their diets and have discussions on WeChat Moments. This helps improve students’ ability to apply nutritional knowledge to real life, which is an important foundation for their nutritional counseling abilities. During the sharing process, students progressively acquire the skill to analyze food nutrition from a professional perspective and offer rational dietary suggestions to others, thereby honing their nutritional counseling abilities. Throughout this process, students perceive themselves as the protagonists of learning, leading to a stronger learning awareness. Awareness influences perception and subsequently modifies behavior, underlining the significance of cultivating learning awareness during the teaching process26. Learning awareness and the willingness to continue learning are essential for augmenting nutritional counseling capabilities. A more pronounced learning awareness and a greater willingness to continue learning impel individuals to actively pursue a diverse range of nutrition-related knowledge. Simultaneously, they are more inclined to proactively engage in practical activities and conduct self-reflection post-practice. Through such self-reflection, they can continuously refine their consulting strategies and practical experiences.
For each chapter test, the main part comprised the content of the respective chapter, with a portion also covering that of previous chapters. As presented in Table 2, significant differences were detected in the first four chapter tests, while no differences emerged in the last three. A potential explanation could be that sharing on WeChat Moments during the first three chapters of blended teaching enabled students to apply their learning flexibly, leading to a more profound understanding and better test results. The fourth chapter initiated with traditional teaching; nevertheless, the influence of blended teaching was still evident. Moreover, the p-value for comparing the test scores in Chap. 4 was 0.05. One study reported that students with excellent academic performance gave higher evaluations regarding the quality of education in the course40. However, our findings suggested that students’ academic performance was not associated with the quality of education but rather with their willingness to further study (Table 5). In other words, students’ academic performance and the quality of education are independent41. The lack of significant differences in final exam grades between groups may reflect the limitations of traditional assessment methods in capturing practical competencies. This also reminds us that the evaluation of teaching quality should not solely rely on academic achievements. Future research should explore competency-based assessments to better align evaluation with real-world clinical demands.
This study was subject to several limitations. Firstly, notwithstanding its prospective nature, a causal analysis remained infeasible. Secondly, in the nutrition course, the teaching approach was bifurcated into blended teaching and traditional teaching solely for the first three chapters, with the last four chapters exclusively adopting traditional teaching. For future studies, it was advisable to incorporate clinical examples for online exchanges in light of the content of the latter four chapters. Finally, during the practical implementation, an imbalance in student participation might have emerged. Some students might have exhibited a higher level of active engagement in online sharing and discussions, while others remained relatively passive. In subsequent research endeavors, teachers could enhance student participation by devising explicit rules, furnishing personalized guidance and offering encouragement, thereby facilitating a more optimal integration of theory and practice. Future research should prioritize hybrid models that integrate virtual simulations (e.g., digital patient scenarios) with hands-on practicums to bridge foundational knowledge and clinical applications. Additionally, leveraging artificial intelligence for personalized feedback in digital platforms could optimize self-directed learning.
The amalgamation of blended teaching and real-life scenarios bears substantial merits in augmenting educational quality. Although it exhibits no significant influence on the final course grades, it conspicuously augments students’ willingness to continue learning, self-directed learning awareness, as well as nutritional counseling capabilities. These innovative pedagogical strategies hold great promise for implementation in a broader spectrum of universities, thereby significantly bolstering nursing students’ self-directed learning ability and nutritional counseling capabilities, which are of utmost importance for elevating the quality of care and improving clinical prognoses.
Data availability
The data that support the findings of this study can be provided by the corresponding author upon reasonable request.
References
-
Hao, X. et al. Application of digital education in undergraduate nursing and medical interns during the COVID-19 pandemic: A systematic review. Nurse Educ. Today. 108, 105183. https://doi.org/10.1016/j.nedt.2021.105183 (2022).
Google Scholar
-
Meum, T. T., Koch, T. B., Briseid, H. S., Vabo, G. L. & Rabben, J. Perceptions of digital technology in nursing education: A qualitative study. Nurse Educ. Pract. 54, 103136. https://doi.org/10.1016/j.nepr.2021.103136 (2021).
Google Scholar
-
Tudor Car, L. et al. Digital education for health professionals: An evidence map, conceptual framework, and research agenda. J. Med. Internet Res. 24, e31977. https://doi.org/10.2196/31977 (2022).
Google Scholar
-
Michener, A., Fessler, E., Gonzalez, M. & Miller, R. K. The 5 m’s and more: A new geriatric medical student virtual curriculum during the COVID-19 pandemic. J. Am. Geriatr. Soc. 68, E61–E63. https://doi.org/10.1111/jgs.16855 (2020).
Google Scholar
-
Zhou, T., Huang, S., Cheng, J. & Xiao, Y. The distance teaching practice of combined mode of massive open online course Micro-Video for interns in emergency department during the COVID-19 epidemic period. Telemed J. E Health. 26, 584–588. https://doi.org/10.1089/tmj.2020.0079 (2020).
Google Scholar
-
Alpert, J. B., Young, M. G., Lala, S. V. & McGuinness, G. Medical student engagement and educational value of a remote clinical radiology learning environment: Creation of virtual Read-Out sessions in response to the COVID-19 pandemic. Acad. Radiol. 28, 112–118. https://doi.org/10.1016/j.acra.2020.09.011 (2021).
Google Scholar
-
Jowsey, T., Foster, G., Cooper-Ioelu, P. & Jacobs, S. Blended learning via distance in pre-registration nursing education: A scoping review. Nurse Educ. Pract. 44, 102775. https://doi.org/10.1016/j.nepr.2020.102775 (2020).
Google Scholar
-
Du, L. et al. Blended learning vs traditional teaching: the potential of a novel teaching strategy in nursing education—a systematic review and meta-analysis. Nurse Educ. Pract. 63, 103354. https://doi.org/10.1016/j.nepr.2022.103354 (2022).
Google Scholar
-
Leidl, D. M., Ritchie, L. & Moslemi, N. Blended learning in undergraduate nursing education—A scoping review. Nurse Educ. Today 86, 104318. https://doi.org/10.1016/j.nedt.2019.104318 (2020).
Google Scholar
-
Li, C., He, J., Yuan, C., Chen, B. & Sun, Z. The effects of blended learning on knowledge, skills, and satisfaction in nursing students: A meta-analysis. Nurse Educ. Today 82, 51–57. https://doi.org/10.1016/j.nedt.2019.08.004 (2019).
Google Scholar
-
Yin, B. & Yuan, C. H. Precision teaching and learning performance in a blended learning environment. Front. Psychol. 12, 631125. https://doi.org/10.3389/fpsyg.2021.631125 (2021).
Google Scholar
-
Cui, C., Li, Y., Geng, D., Zhang, H. & Jin, C. The effectiveness of evidence-based nursing on development of nursing students’ critical thinking: A meta-analysis. Nurse Educ. Today 65, 46–53. https://doi.org/10.1016/j.nedt.2018.02.036 (2018).
Google Scholar
-
De Gagne, J. C., Kim, S. S., Schoen, E. R. & Park, H. K. Assessing the impact of video-based assignments on health professions students’ social presence on web: case study. JMIR Med. Educ. 4, e11390. https://doi.org/10.2196/11390 (2018).
Google Scholar
-
Hickmann, A. K., Ferrari, A., Bozinov, O., Stienen, M. N. & Ostendorp, C. Neurosurgery resident training using blended learning concepts: Course development and participant evaluation. Neurosurg. Focus 53, E13. https://doi.org/10.3171/2022.5.FOCUS22193 (2022).
Google Scholar
-
Brereton, S. et al. A blended learning perineal suturing programme for midwifery students: An evaluative descriptive study. Nurse Educ. Pract. 64, 103453. https://doi.org/10.1016/j.nepr.2022.103453 (2022).
Google Scholar
-
Balakrishnan, A. et al. Effectiveness of blended learning in pharmacy education: An experimental study using clinical research modules. PLoS One 16, e0256814. https://doi.org/10.1371/journal.pone.0256814 (2021).
Google Scholar
-
Huang, T. H., Liu, F., Chen, L. C. & Tsai, C. C. The acceptance and impact of Google classroom integrating into a clinical pathology course for nursing students: A technology acceptance model approach. PLoS One 16, e0247819. https://doi.org/10.1371/journal.pone.0247819 (2021).
Google Scholar
-
Cao, W. et al. Massive open online Courses-based blended versus face-to-face classroom teaching methods for fundamental nursing course. Medicine 100, e24829. https://doi.org/10.1097/MD.0000000000024829 (2021).
Google Scholar
-
Blissitt, A. M. Blended learning versus traditional lecture in introductory nursing pathophysiology courses. J. Nurs. Educ. 55, 227–230. https://doi.org/10.3928/01484834-20160316-09 (2016).
Google Scholar
-
Devi, B., Khandelwal, B. & Das, M. Comparison of the effectiveness of Video-assisted teaching program and traditional demonstration on nursing students learning skills of performing obstetrical palpation. Iran. J. Nurs. Midwifery Res. 24, 118–123. https://doi.org/10.4103/ijnmr.IJNMR_35_18 (2019).
Google Scholar
-
Wang, S., Liu, K., Tang, S. & Chen, Q. Instruments for measuring patient health education competence among nursing personnel: A COSMIN-based systematic review. Nurse Educ. Pract. 72, 103798. https://doi.org/10.1016/j.nepr.2023.103798 (2023).
Google Scholar
-
Wang, S., Liu, K., Shi, Z., Chen, Q. & Tang, S. Instruments for measuring patient health education competence among nursing personnel: protocol for a COSMIN-based systematic review. BMJ Open 13, e072905. https://doi.org/10.1136/bmjopen-2023-072905 (2023).
Google Scholar
-
Dogan, E. I. K., Borgen, I., Ekiz, P. & Wesseltoft-Rao, N. Nutrition education for nursing students: A scoping review. Nurse Educ. Today. 144, 106460. https://doi.org/10.1016/j.nedt.2024.106460 (2025).
Google Scholar
-
Wang, G. et al. Interventions to improve patient health education competence among nursing personnel: A scoping review protocol. BMJ Open. 14, e087015. https://doi.org/10.1136/bmjopen-2024-087015 (2024).
Google Scholar
-
Antón-Solanas, I. et al. Nursing lecturers’ perception and experience of teaching cultural competence: A European qualitative study. Int. J. Environ. Res. Public. Health. https://doi.org/10.3390/ijerph18031357 (2021).
-
Anton-Solanas, I. et al. Nursing students’ experience of learning cultural competence. PLoS One. 16, e0259802. https://doi.org/10.1371/journal.pone.0259802 (2021).
Google Scholar
-
Almendingen, K., Knutsen, I. R., Hjerpaasen, K. J., Henjum, S. & Hakestad, K. A. It enables Us to reflect more on nutrition: A mixed methods cross-sectional study on preclinical digital training in nurse education. Educ. Sci. 13, 32 (2023).
-
Mancin, S., Soekeland, F., Morenghi, E., Andreoli, D. & Mazzoleni, B. Enhancing the teaching of nutrition for nursing students: engagement in class through a digital learning environment. Teach. Learn. Nurs. 19, e229–e234. https://doi.org/10.1016/j.teln.2023.11.001 (2024).
Google Scholar
-
Thang, C. K. et al. Impact of a teaching kitchen curriculum for health professional trainees in nutrition knowledge, confidence, and skills to advance obesity prevention and management in clinical practice. Nutrients 15, 4240 (2023).
Google Scholar
-
Deng, A., Wang, Y., Zhang, T. & Chen, A. Learning to teach again: What professional development approach matters?? J. Teach. Phys. Educ. 41, 78–87. https://doi.org/10.1123/jtpe.2020-0121 (2022).
Google Scholar
-
Bahn, D. Social learning theory: Its application in the context of nurse education. Nurse Educ. Today 21, 110–117. https://doi.org/10.1054/nedt.2000.0522 (2001).
Google Scholar
-
Marsh, H. W. & SEEQ A reliable, valid, and useful instrument for collecting students’ evaluations of university teaching. Br. J. Educ. Psychol. 52, 77–95 (1982).
Google Scholar
-
Ganatra, S. et al. Perceived effectiveness and applicability of Think-Pair-Share including storytelling (TPS-S) to enhance clinical learning. Teach. Learn. Med. 33, 184–195. https://doi.org/10.1080/10401334.2020.1811094 (2021).
Google Scholar
-
Griffiths, A., Sun, A., Feinberg, J., Wiesel, O. & Rhee, R. The whiteboard time out: A novel tool to improve resident learning in the operating room. J. Surg. Educ. 80, 912–921. https://doi.org/10.1016/j.jsurg.2023.04.003 (2023).
Google Scholar
-
Williamson, S. N. Development of a self-rating scale of self-directed learning. Nurse Res. 14, 66–83. https://doi.org/10.7748/nr2007.01.14.2.66.c6022 (2007).
Google Scholar
-
Sørensen, K. et al. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public. Health 12, 80. https://doi.org/10.1186/1471-2458-12-80 (2012).
Google Scholar
-
Fatani, T. H. Student satisfaction with videoconferencing teaching quality during the COVID-19 pandemic. BMC Med. Educ. 20, 396. https://doi.org/10.1186/s12909-020-02310-2 (2020).
Google Scholar
-
Tudor Car, L. et al. Digital Problem-Based learning in health professions: Systematic review and meta-analysis by the digital health education collaboration. J. Med. Internet Res. 21, e12945. https://doi.org/10.2196/12945 (2019).
Google Scholar
-
Pimdee, P., Sukkamart, A., Nantha, C., Kantathanawat, T. & Leekitchwatana, P. Enhancing Thai student-teacher problem-solving skills and academic achievement through a blended problem-based learning approach in online flipped classrooms. Heliyon 10, e29172. https://doi.org/10.1016/j.heliyon.2024.e29172 (2024).
Google Scholar
-
Greenwald, A. G. Validity concerns and usefulness of student ratings of instruction. Am. Psychol. 52, 1182–1186 (1997).
Google Scholar
-
Moraros, J., Ashrafi, A., Yu, S., Banow, R. & Schindelka, B. Correction to: Flipping for success: Evaluating the effectiveness of a novel teaching approach in a graduate level setting. BMC Med. Educ. 17, 203. https://doi.org/10.1186/s12909-017-1027-8 (2017).
Google Scholar
Acknowledgements
The authors would like to thank all students, who volunteered to participate in the study. This work was supported by Anhui Province Quality Engineering Project [Grant number 2020jyxm2086, 2022jyxm1699, 2023ylyjh046, 2023cxtd170]; and Wannan Medical College Quality Engineering Project [Grant number 2021jyxm43].
Author information
Authors and Affiliations
Contributions
A.S.W.: Writing review & editing, Writing original draft, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. J.J.W.: Writing review & editing, Writing original draft, Project administration, Methodology, Formal analysis. T.J.Z.: Writing original draft, Methodology, Investigation, Formal analysis, Data curation. Y.C.: Writing original draft, Methodology, Funding acquisition, Formal analysis, Conceptualization. B.B.Q.: Writing original draft, Methodology, Formal analysis, Conceptualization. Y.X.: Writing original draft, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Y.L.J.: Writing review & editing, Project administration, Methodology, Funding acquisition, Formal analysis, Conceptualization. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
Reprints and permissions
About this article
Cite this article
Wang, A., Wan, J., Zhang, T. et al. Blended nutrition education with real-life scenarios enhances learning and nutritional counseling capabilities in nursing students.
Sci Rep 15, 11570 (2025). https://doi.org/10.1038/s41598-025-96144-x
-
Received: 06 December 2024
-
Accepted: 26 March 2025
-
Published: 04 April 2025
-
DOI: https://doi.org/10.1038/s41598-025-96144-x
Keywords
- Blended nutrition education
- Nursing student
- Real-life scenarios
- Educational quality
- Nutritional counseling capabilities