Study design and recruitment
The two-phase COHESION Study is a pan-Canadian prospective cohort study. COHESION Phase 1 was conducted between May 2020 and September 2021. COHESION Phase 2 will be launched in May 2022. All Phase 1 participants will be invited to participate in Phase 2, and additional recruitments (n = 10,000) will be done.
After consenting to participate to the study, participants are invited to fill a short eligibility questionnaire. Inclusion criteria are being aged 15 years or above, currently residing in Canada, and reading or speaking English or French. Eligible participants are then invited to complete a baseline questionnaire.
The recruitment for COHESION Phase 1 was launched on May 11 2020. We used a combination of methods that have proven successful from previous experience in recruiting population-based research project samples [33], including media communication (e.g., newspaper articles, radio interviews), social media promotion (e.g., Facebook, Twitter, Instagram, and LinkedIn), and outreach through partners’ local networks (e.g., local health authorities that relayed the study on their website or through their newsletters).
For COHESION Phase 2, we will further use quota sampling at the health region level, based on 2016’s Census data (i.e., age composition, gender, income, educational attainment, and ethnic background). We engaged Potloc Inc., a tech-enabled consumer research company that conducts survey sampling through social networks (Facebook, Twitter, Instagram, LinkedIn), for geo-targeting of respondents based on the sampling quotas. Potloc Inc.’s algorithm will push sociodemographic and geographically targeted online ads to our study until local quotas are attained (targets are monitored daily) and that 10,000 participants have thereby been enrolled. Furthermore, a geographical oversampling (n = 1,000) will be conducted in Nord-de-l’Île-de-Montréal (NIM) territory (Quebec), in partnership with the NIM’s integrated health and social services center (CIUSSS-NIM).
Enrollment and participation in the two-phase COHESION Study are voluntary, and a raffle of three prizes ($100 gift cards) is drawn every month for active participants for the duration of the study.
Data collection
In the subsequent paragraphs, we will explicitly indicate whether the information discussed pertains to Phase 1, Phase 2, or both phases to provide clarity for the reader.
Involvement options
For both study’s phases, two levels of involvement are proposed. Participants can opt for: (i) participating in the online self-administered questionnaires only (baseline + invitation to follow up questionnaires); or (ii) participating in the questionnaires and downloading a mobile phone application to provide additional active and passive data (cf. 3.2.5).
Baseline questionnaires
Through the COHESION Study Phase 1 baseline questionnaire (35–45 min), participants report on: their sociodemographic characteristics (e.g., gender, ethnic or cultural background, education level, employment status, income, relationship status, and household composition); housing condition (e.g., house tenure, dwelling type and size, outdoor space) and satisfaction; physical (e.g., chronic disease diagnosis) and mental health conditions (e.g., anxiety and depression), and substance use (alcohol, tobacco, vape, and cannabis); COVID-19 infection status, vulnerability towards COVID-19, perception of- and compliance with COVID-19 mitigation measures, and pre-pandemic employment, income, substances use, loneliness, resilience, and social interactions. Additionally, a map-based questionnaire collects data on activity locations and social contacts (cf. Fig. 2). For parents, a supplementary module on mental health and perceptions of COVID-19 mitigation measures concerning adolescents and children who live in the household is administered (participants answer on behalf of children in their household).
The COHESION Study Phase 2 baseline questionnaire will consist in one core (10 min) and two optional complementary Sect. (15 min each). The core baseline questionnaire includes: sociodemographic characteristics and key housing conditions; COVID-19 vaccination status, perceptions of COVID-19 pandemic and related mitigation measures; standardized modules assessing general health (first item of the 12-item Short-Form Health Survey) [34], well-being (5-item World Health Organization Well-Being Index, WHO-5 Index) [35], sleep credit (Pittsburgh Sleep Quality Index, PSQI, 4 items only) [36], and psychological distress (Psychological Distress Scale, Kessler-6) [37]; and an outdoor mobility and social interactions module. Optional complementary baseline sections include the map-based questionnaire on activity locations and social contacts (cf. 3.2.4) and additional in-depth questions on relevant themes: additional items retrieved from the Phase 1 baseline questionnaire (it means all items not already included in the Phase 2 core baseline questionnaire); standardized modules on loneliness (University of California Los Angeles, UCLA, 3-item loneliness score) [38], anxiety symptoms (7-item Generalized Anxiety Disorder, GAD-7) [39], depression symptoms (9-item Patient Health Questionnaire, PHQ-9) [40], resilience (6-item Brief Resilience Scale) [41], sense of belonging (Canada Community Health Survey, CCHS) [42], and physical activity (Godin Leisure-Time Exercise) [43]; items for assessing conspiracy beliefs.
Slightly shorten versions of the Phase 2 baseline questionnaires (i.e., excluding questions about birth, cultural background, etc.) have been provided for participants coming from Phase 1 and wishing going on Phase 2.
Follow-up questionnaires
Follow-up questionnaires of the COHESION Study are short questionnaires (15 min). For Phase 1, they were first offered biweekly until August 2020, then monthly. COVID-19-related topics cover infection and/or vaccination status, perceived vulnerability, perception of and compliance with mitigation measures, position regarding vaccination, and conspiracy beliefs. Health-related questions focus on general health (SF-12, first item) [34], well-being (WHO-5 Index) [35], sleep credit (PSQI, 4 items only) [36], loneliness (UCLA 3-item loneliness score) [38], anxiety symptoms (GAD-7) [39], depression symptoms (PHQ-9) [40], psychological distress (Kessler-6) [37], and sense of belonging (CCHS) [42] (Table 1). Employment status, household income, and substance use are also documented. Additionally, participants are asked at each follow-up about any changes concerning their place of residence and housing conditions. Supplementary module on mental health and perception of COVID-19 mitigation measures concerning children or adolescents living at home is administered when applicable.
For Phase 2, follow-up questionnaires will be split in a core (‘light’) and an optional complementary (‘complete’) sections, and will be offered every two months. It will include the same questions as for Phase 1, adding a standardized module for assessing physical activity (Godin Leisure-Time Exercise Questionnaire) [43].
Questions can vary between follow-ups, depending on the situation and priorities raised by the research team and our public health partners. Thus, these additional themes can focus on health insecurity (i.e., access to health care, prescriptions and medicine) [44], sleep troubles (PSQI) [36], food insecurity (10-item Health Canada Household Food Security Module) [45], and children’s difficulties (if any) [45].
For Phase 1, follow-up questionnaire waves are named according to their week and year of release (for instance, “20/26” for the follow-up questionnaire proposed to participants in the 26th week of 2020).
Use of VERITAS-Social to collect daily mobility and social interaction data
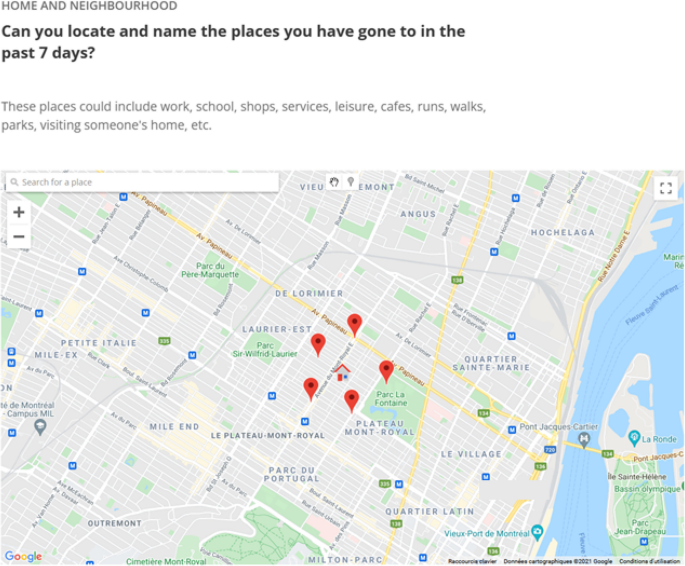
One of the specificities of COHESION is that it integrates, in baseline and follow-up questionnaires of the two phases, the Visualization and Evaluation of Route Itineraries, Travel destinations, Activity spaces and Social interactions (VERITAS-Social) questionnaire. For COHESION, it was adapted to locate a possible list of up to 20 activities carried out during the past seven days (Fig. 2). As previously described, VERITAS-Social is an interactive map-based questionnaire that jointly collects an individual’s social network and activity locations [46]; it is an adaptation of the VERITAS tool, an interactive questionnaire for geo-locating places, and related information of interest (e.g., frequency of visit, transportation modes used) [47]. It uses a Google Map module to facilitate the location of activity places. The social module asks if an activity location is generally visited alone or with someone else; participants can identify one or more individuals, or a group of people (see S1a-b Figs). In other words, it is a name generator that identifies network members based on their co-presence at reported destinations [48]. Data on network members include age, gender, type of relationship (e.g., friend, acquaintance), frequency of interactions, and duration of the relationship; for groups, data includes the number of people in the group, and the duration of the relationship.

Collecting data on living and activity places with VERITAS-Social. Screenshot from the VERITAS application (map-based survey tool – permission given from Polygon Inc.) for a fictional participant; the house icon locates the participant’s residential address and the pin icons symbolize the visited places located by the participant
Once all activities, corresponding locations, and all people with whom these activities are carried out have been reported, participants are asked to identify members of their social network from whom they receive support or with whom they enjoy spending time with, including members who may not have been reported among the people seen at usual activity venues. Finally, participants were able to indicate interpersonal relationships between network members (i.e., who knows whom), and whether some specific individuals belonged to documented groups.
In Phase 1, the VERITAS-Social questionnaire was mandatory for all participants. To optimize the representativeness of our sample, we adapted our approach in Phase 2 by making this questionnaire optional.
Optional mobile application
Participants enrolling in the mobile phone arm of the study were invited to download Ethica Data mobile application (cf. 3.2.1), used successfully in previous research projects [49]. Once installed and launched, the application passively monitors location and mobility (e.g., stationary, in vehicle, walking, or biking) using GPS data (1 min of data collected every 5 min), physical activity (step counter), and social contacts (other smartphones), derived from listings of other Bluetooth discoverable devices in the participant’s surroundings (for more details see [50]). The app further prompts participants to complete Ecological Momentary Assessment (EMA) questionnaires three times a day for one week every month. EMA questionnaires include short self-reports (< 1 min) on well-being, sleep, mood (Short Mood Scale, 6 items) [51], and social interactions (see S2 Fig).
Environmental data
Because some of the data collected is spatial (e.g. place of residence, VERITAS-Social locations, mobile app GPS data), we are able to add area-level environmental data to our dataset. This allows to explore links between individual-level measures and social and environmental contextual conditions. Numerous environmental datasets covering Canada are available through the Canadian Urban Environmental Health Research Consortium (CANUE), which can be linked to our dataset using the 6-position postal code – a key identifier for all participants.
Contextual variables of interest include measures of neighborhood deprivation, such as the Material and Social Deprivation Indices (MSDI; data 2016) available at the Canadian Census dissemination area level (i.e., the smallest Canadian standard geographic area, with a population of 400 to 700 persons) [52]. These two composite indexes combine Census data on educational attainment, employment ratio, average income, and household composition.
The urbanization degree is measured using Statistics Canada classification (at the four-digit code area level; data 2016), based on the number of inhabitants in population centers [53]. “Small”, “medium” and “large” urban population centers correspond to areas embracing between 1,000 and 29,999, between 30,000 and 99,999, and 100,000 and more inhabitants, respectively, while “rural area” is a residual value gathering all areas located outside population centers.
Greenness is evaluated using the growing season Normalized Difference Vegetation Index (NDVI) (at the six-digit code area level; data 2019), based on Landsat 8 satellite data [54, 55].
Area-level walkability is measured using the Canadian Active Living Environments (CAN-ALE) database [56].
Additional localized and temporalized data on COVID-19 pandemic conditions, including lockdowns, curfews, vaccination plan, number of cases, and emergence of variants is also available through the Canadian Institute for Health Information (CIHI) compilation [57].
Ethics and data management plan
Before completing the eligibility questionnaire, potential participants are first invited to read the consent form and provide an electronic written consent to participate in the study. Informed consent was then obtained from all subjects and/or their legal guardian(s). In Phase 2, a second consent will be required from participant wishing to register for the prospective follow-ups after having completed baseline questionnaire. Phase 1 COHESION was approved by the ethics board of the Centre de Recherche du Centre Hospitalier de l’Université de Montréal (CRCHUM; MP-02-2021-8924) and by the Public Health Agency of Canada (PHAC) ethical review board (REB 2020-016P). Phase 2 COHESION was approved by both the ethics board of the Centre Intégré Universitaire de Santé et de Services Sociaux du Nord-de-l’Île-de-Montréal (CIUSSS-NIM ; 2022–2327) and PHAC (REB 2020-016P). All methods used in the project were carried out in accordance with relevant guidelines and regulations.
For data security and privacy proposal, all data are hosted on Compute Canada servers with secondary backups on hospital-grade internal servers. All data has been stripped from any personally identifying information, with only the principal investigator being able to track the records back to one participant. Researchers can access anonymized individual level records by connecting directly through a Secure Shell (SSH) to the database hosted on Compute Canada (a SSH allows remote machines accessing data in a secure way since the connection is encrypted). They can also access aggregated data for analysis through a secure online platform hosted by Tableau [58]. A document listing all the data management policies governing data access and storage has been submitted to the ethic board for approval.