Study population and ethics
NHANES is a nationwide campaign launched by National Center for Health Statistics (NCHS) that mainly focuses on the health and nutritional condition of the noninstitutionalized US civilians at two-year intervals, and whose aim is to obtain a comprehensive knowledge of contemporary disease profiles and to provide references for formulating public health policies. All of the NHANES data is accessible to the public and can be downloaded freely through: https://www.cdc.gov/nchs/nhanes/index.htm. In this study, cross-sectional data of 101,316 participants from ten consecutive cycles of the NHANES (1999–2018) were initially included. The exclusion criteria were set as our previous studies using NHANES database to exploring risk factors of hypertension: (1) participants aged < 18 or ≥ 80 years (n = 33,272); (2) participants who were pregnant (n = 1,592); (3) participants without relevant information on dietary intake or hypertension (n = 18,783); (4) participants whose estimated glomerular filtration rate (eGFR) < 60 ml/min/1.73m2 (n = 2,661) [22,23,24]. After manual data filtration, we ultimately selected a total of 42,391 participants for subsequent analyses. The study protocol has gained approval from the NHANES Institutional Review Board, with informed consent being obtained from all the participants. A detailed flow chart of study participant recruitment was presented in Fig. 1.
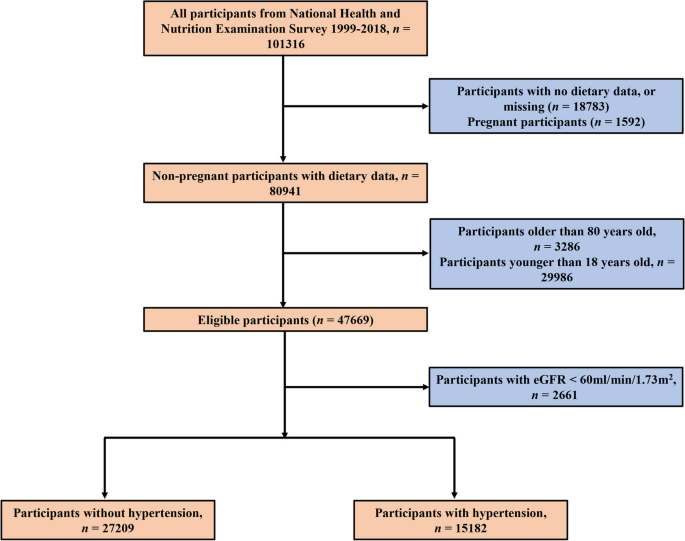
A detailed flow chart of participant recruitment
Assessment of dietary quality
Since NHANES surveys are a series of large-scale population-based campaigns, it is necessary to collect dietary information rapidly and conveniently. To this end, 24-h dietary data — including the types and amounts of food and drinks consumed during the 24-h period prior to the interview in the mobile examination center (MEC) — was collected by trained interviewers following a standardized protocol, and was then used to calculate the HEI-2015 score as previously reported [23, 25]. According to the 2015–2020 DGA, a total of 13 dietary components taken into account in the HEI-2015 scoring system can be divided into two categories, one of which comprises nine adequacy components that are encouraged to be adequately consumed (Total Fruits, Whole Fruits, Total Vegetables, Greens and Beans, Whole Grains, Dairy, Total Protein Foods, Seafood and Plant Proteins, and Fatty Acids), and the other one of which is composed of four moderation components, the recommended intake of which should be strictly confined within a modest range (Refined Grains, Sodium, Added Sugars, and Saturated Fats). Each dietary component is assigned a maximal score of 5 or 10, which was then summed up to generate an overall HEI-2015 score, the theoretical reference range of which is 0–100. A dietary pattern advocating for higher intake of adequacy components as well as lower intake of moderation components usually corresponds to a higher HEI-2015 score, which is commonly indicative of a better quality of the diet [12].
Assessment of hypertension
Hypertension can be defined based on either self-reported previous diagnosis by a physician or blood pressure measured during physical examination. A standardized procedure recommended by American Heart Association was conducted for blood pressure measurements. After sitting in a comfortable position for at least 5 min, three single measurements were performed by well-trained clinicians equipped with mercury sphygmomanometers at half-minute intervals. To mitigate accidental errors caused by blood pressure fluctuations, the mean value of all three readings was calculated and recorded as one participant’s blood pressure. Anyone who met at least one of the criteria listed below was considered as having hypertension: (1) Average systolic blood pressure (SBP) ≥ 140 mmHg; (2) Average diastolic blood pressure (DBP) ≥ 90 mmHg; (3) Self-reported diagnosis of hypertension; (4) Current use of anti-hypertensive medications [26]. More relevant information about blood pressure measurement is available on the NHANES website (http://www.cdc.gov/nchs/data/nhanes/pe.pdf). To be noted, use of self-reported measures are prone to recall bias, which may have an impact on the interpretation of the data.
Covariates
Being based on previous publications and biological considerations, we collected as much covariates with known confounding effects on hypertension as possible. Demographic features including age, sex, race/ethnicity, educational level, smoking status, and alcohol consumption were obtained by standardized questionnaires and face-to-face interviews. Physical examination and laboratory tests were performed by experienced medical workers step by step in the MEC.
Race/ethnicity were divided into five categories: non-Hispanic White, non-Hispanic Black, other Hispanic, Mexican American, and other races. The following educational levels were included: below high school, high school, and above high school. Participants who smoked over 100 cigarettes throughout their lifetime were defined as smokers, regardless of whether he/she had quitted smoking at the time of interview [27], and those consuming at least 12 drinks during the year preceding the survey were considered alcohol drinkers [28]. Body mass index (BMI), calculated as weight in kilograms (kg) divided by the square of height in meters (m2), is widely used for estimating overweight/obesity status. A BMI score greater than 25 and 30 is recognized as the major diagnostic criteria of overweight and obesity in clinical practice, respectively [29]. Fasting blood glucose (FBG) and serum concentrations of glycated hemoglobin (HbA1c), triglyceride (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C) were examined by standardized laboratory tests. For calculating eGFR, NHANES investigators applied a formula developed by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) in which variables including age, sex, race/ethnicity, and serum creatinine (SCr) were incorporated to adapt to different populations [30].
Besides, diabetes was another important confounder that may have an impact on hypertension and other cardiovascular diseases [31, 32]. Anyone who provided a previous diagnosis of diabetes by a physician or health professional was defined as patients with diagnosed diabetes, while those without diagnosed diabetes but with a HbA1c level 6.5% (47.5 mmol/mol) or higher, FPG level 126 mg/dL (7.0 mmol/L) or higher, or 2-h oral glucose tolerance test (OGTT) plasma glucose 200 mg/dL or higher (11.1 mmol/L) tested by laboratory examinations were classified as having undiagnosed diabetes. Participants with diagnosed diabetes or undiagnosed diabetes were both considered diabetic patients [33, 34].
Statistical analysis
Since NHANES survey employed a series of complex sampling designs, we took into account the sample weights corresponding to different research periods in our analytic methods to yield accurate estimates of health-related statistics [35,36,37,38]. Continuous variables were presented in the form of weighted mean and standard deviation (SD), whereas categorical variables were expressed as frequencies and percentages. For the purpose of detecting differences in baseline characteristics between participants with and without hypertension, continuous and categorical variables were compared using student’s t-test and chi-square test, respectively. The HEI-2015 score was categorized into four quartiles (Q1: HEI-2015 < 40.3; Q2: 40.3 ≤ HEI-2015 < 49.6; Q3: 49.6 ≤ HEI-2015 < 58.2; Q4: HEI-2015 ≥ 58.2), with the first quartile (Q1) being the reference quartile.
We used a variety of multivariate logistic regression models to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) for detecting the association of HEI-2015 with hypertension. Adjustments for age and study circle was performed in Model I; Model II was further adjusted for sex and race/ethnicity; Model III was adjusted for additional confounders including educational level, smoking status, alcohol consumption, diabetes, and eGFR in addition to those adjusted in Model II. We also applied restricted cubic spline (RCS) regression with 3 knots (10th, 50th, and 90th percentiles) to examine the nonlinearity of the association between HEI-2015 and hypertension. Subgroup analyses in terms of age, sex, race/ethnicity, BMI, diabetes were conducted to verify whether the association between HEI-2015 and hypertension remained stable across different subgroups. A sensitivity analysis was also performed to validate the stability of the association between HEI-2015 and hypertension. R software version 4.1.6 (http://www.R-project.org, The R Foundation, Vienna, Austria) was used for all statistical analyses, and a two-tailed P-value < 0.05 was considered statistically significant.